OMT EFFECT IN ESSENTIAL HYPERTENSION
Osteopathic manipulation as a complementary
treatment for the prevention of cardiac
complications: 12-Months follow-up of intima media
and blood pressure on a cohort affected
by hypertension
Francesco Cerritelli, MS, DO
, Fabrizio Carinci, MS
,
Gianfranco Pizzolorusso, DO
, Patrizia Turi, DO
,
,
Cinzia Renzetti, MD, DO
, Felice Pizzolorusso, DO
,
Francesco Orlando, DO
, Vincenzo Cozzolino, MD, DO
,
Gina Barlafante, MD, DO
a
European Institute for Evidence Based Osteopathic Medicine (EBOM), Viale Unita` d’Italia 1, 66100 Chieti, Italy
b
AIOT Research Institute, Pescara, Italy
Received 18 September 2009; received in revised form 5 March 2010; accepted 20 March 2010
KEYWORDS
Cardiovascular
disorders;
Intima-media thickness;
Systolic/diastolic blood
pressure;
Osteopathic
manipulative treatment
Summary
Background: Aim of the present study was to investigate the association between
osteopathic treatment and hypertension.
Methods: The design was a non-randomized trial including consecutive subjects affected by
hypertension and vascular alterations, using pre
epost differences in intima-media thickness,
systolic and diastolic blood pressure as primary endpoints.
Statistical analysis was based on univariate t tests and multivariate linear regression.
Results: A total of N
Z 31 out of N Z 63 eligible subjects followed by a single cardiologist
received osteopathic treatment in addition to routine care. Clinical measurements were
recorded at baseline and after 12 months.
Univariate analysis found that osteopathic treatment was significantly associated to an
improvement in all primary endpoints. Multivariate linear regression showed that, after adjust-
ing for all potential confounders, osteopathic treatment was performing significantly better for
* Corresponding author. Via Prati 29, 65124 Pescara, Italy. Tel.:
þ39 339 4332801; fax: þ39 0873 380520.
E-mail address:
(F. Cerritelli).
a v a i l a b l e a t w w w . s c i e n c e d i r e c t . c o m
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / j b m t
Journal of Bodywork & Movement Therapies (2011) 15, 68
e74
1360-8592/$ - see front matter
ª 2010 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jbmt.2010.03.005
intima-media thickness (delta between pre
epost differences in treated and control groups:
0.517; 95% c.i.: 0.680, 0.353) and systolic blood pressure (4.523; 6.291, 2.755),
but not for diastolic blood pressure.
Conclusion: Our study shows that, among patients affected by cardiovascular disorders, oste-
opathic treatment is significantly associated to an improvement in intima-media and systolic
blood pressure after one year. Multicentric randomized trials of adequate sample size are
needed to evaluate the efficacy of OMT in the treatment of hypertension.
ª 2010 Elsevier Ltd. All rights reserved.
Background
The relation between endothelial wall modifications (
), and change of the endothelial carotid wall
(
Simon et al., 2002; Labropoulos et al., 2000; Safar et al.,
) on hypertension is well documented by the scien-
tific literature. The degeneration of the endothelial layer is
associated to a variation of metabolic processes in vessels,
determining plaques growing (
) and variations
in the hemodynamic of blood fluid (
) that may trigger the atherosclerosis process
(
) through an increase in intima-media
thickness (IMT) (
The condition of the vascular wall can be altered by
endogenous factors, e.g. genetic alterations, or exogenous
determinants, which can include many potential aspects of
the complex interaction between the subject and the outer
environment. Behavioural factors e.g. a high level of
physical activity are significantly associated to a decreased
incidence of atherosclerosis (
Goldsmith et al., 2000; Carter et al., 2003; Tanaka et al.,
2002
). Psycho-physical conditions e.g. stress, through
their influence on the autonomic nervous functions, may
lead
to
alterations
of
both
the
arterial
pressure
(
) and the endothelium (
Manipulative techniques may be included in the range of
exogenous factors of potential interest in the prevention of
hypertension and cardiovascular events (
In this field, evidence-based guidelines applied by clin-
ical cardiologists for high risk subjects include continuous
monitoring through the regular measurement of blood
pressure (BP) and the evaluation of IMT and the arterial wall
(
A
thorough
research
of
the
scientific
literature,
including relevant papers from integrative and comple-
mentary medicine journals, shows that the potential role of
osteopathic manipulative treatment (OMT) has been
already considered in the treatment of hypertension,
mainly as a possible modifier of the relationship between
somatic dysfunctions and hypertension (
Johnston and Golden, 2001; Johnston et al., 1995;
Johnston and Kelso, 1995
).
The aim of the present study was to investigate the
direct association between OMT and hypertension through
the observation of relevant clinical parameters that are
routinely used in clinical practice to prevent long-term
cardiovascular disorders.
Methods
Objectives and endpoints of the study
The main objective of the study was to evaluate the effi-
cacy of OMT on a subgroup of consecutive subjects pre-
senting hypertension and vascular alterations following
cardiologic examination.
Primary endpoints of the study were differences
between treated and control groups in changes from
baseline for IMT and BP (systolic, diastolic) after 12 months.
Study population
The study was coordinated by the Osteopathic Clinical
Centre “AIOT” in the city of Pescara, located in Central
Italy with a population of 120,000.
A private cardiologist was asked to refer to the Centre all
consecutive subjects visited in year 2007 that were meeting
the following inclusion criteria: presence of hypertension,
classified as grade 1
þ according to the specifications of WHO
What is OMT?
Osteopathic manipulative treatment (OMT) is the
process through which osteopaths treat somatic
dysfunctions. Somatic dysfunctions are catalogued as
disease of musculoskeletal system (ICD-9, code 739)
and are identified by TART parameters (see text). OMT
is characterized by different techniques, i.e. myofas-
cial release, craniosacral, High Velocity Low Ampli-
tude (HVLA) manipulation, Balanced Ligamentous
Tension (BLT), Muscle Energy Technique, biodynamic,
strain
ecounterstrain, etc. This wide range of tech-
niques permits the operator to choose the more
appropriate to apply on a patient in a given moment.
During scientific studies, OMT can be used as an
approach, as was done in this study, or as an isolated
technique. The former uses individualized techniques
in relation to the need of the patient while the latter
one employs standardized technique. These reflect
two different ways of utilising OMT. One is based on
effectiveness
e meaning how the use of a global
approach can change outcomes. The second is based
on the efficacy of just one technique, on outcomes.
Osteopathic Manipulative Therapy
69
), and B-ultrasound morphology classified as
II, III, IV (
).
A total of N
Z 72 eligible subjects entered the study.
A subgroup of N
Z 9 patients was considered more severe
and thus excluded from the cohort, due to the presence of
multiple risk factors and/or relevant complications in the
previous 10 years. The assessment was conducted by the
same cardiologist on the basis of the history of renal/retinal
disease, hypercholesterolemia (
>250 mmol/l), diabetes,
metabolic problems (as obesity or X syndrome) and smoking.
Among the 63 patients finally enrolled in the cohort,
N
Z 31 were non-randomly assigned to OMT, and N Z 32
continued to be observed as a control group. All patients
enrolled were invited to conduct in the same visit a series of
baseline instrumental examinations (BP, IMT, BMI, height,
weight, rest heart rate). Patients assigned to OMT were
separately treated by a registered trained osteopath every
fortnight, for a period of one year. A final follow up cardio-
logic visit was scheduled after 12 months to test pre
epost
variation of measurements recorded at baseline.
All subjects expressed their consent to the study and
were followed up by the same cardiologist.
Pharmacological treatment
Antihypertensive treatment was routinely administered to
all patients over 12 months, according to updated evidence-
based guidelines routinely applied by the clinical cardiolo-
gist. Calcium channel blockers (CA
2
þ
), ACE-inhibitors (ACE),
beta-blockers (BB) and diuretics were prescribed either
alone or in combination.
Treatment procedures and specific target
parameters
Osteopathic treatment consisted of a visit during which
a single operator initially performed a series of specific
tests to evaluate the mobility of different parts of the body
), and then treated the patient
focusing on selected targets.
Evaluation represents a key preliminary component of
osteopathic practice. It allows to collect basic information
on tissue characteristics and to highlight the presence of
functional alterations (also known as TART– for Tenderness,
Asymmetry, Range of motion change, Tissue texture change)
in specific areas of the body. Palpation provides essential
knowledge of the structures positioned in regions of the body
that are more subject to changes in the tone of the auto-
nomic nervous system (
), identified by
particular patterns of stiffness/tenderness of the tissues
(muscles, fascias, etc).
In the present study, the following tests (
were performed at each visit: the “spring test”, for dorsal
and lumbar spine; the “F.AB.ER. test” for hips; the “internal
and external rotation test” for arms; and the “six movements
test” for the neck. In each case, a state of initial resistance
denoted the potential presence of somatic dysfunction.
Osteopathic treatment was performed on the part of the
body presenting greater TART modifications applying
fascial, cranial and balanced ligamentous tension tech-
niques (
).
Clinical measurements
All subjects underwent 24-hour ambulatory monitoring
system (Holter) as part of the cardiologic test for hypertension
performed at study entry. In the same visit, clinical
measurements were also performed, including BMI, height,
weight, rest heart rate and a series of instrumental tests for BP
and IMT. All measurements were repeated after 12 months.
Resting BP was measured using a standard sphygmoma-
nometer, with the subject lying in supine rest position for
30 min at the time of ultrasound examination. The retained
value was the average of three consecutive measurements,
rounded to the nearest integer mm/Hg.
Both carotid and femoral arterial bifurcations were
studied to measure IMT in millimetres (mm). All measure-
ments were performed using an ATL Ultramark 4 duplex
scanner with a high-resolution, 7.5-MHz linear transducer.
After localizing the carotid and femoral bifurcations
through a transverse scan, the probe was rotated 90
to
record a longitudinal image of both the anterior and
posterior walls. The carotid artery was evaluated for
a length of about 3 cm (1.5 cm proximal and 1.5 cm distal to
the flow divider). The femoral artery was examined at the
femoral bifurcation and scanned for a length of 3 cm
(1.5 cm proximally and distally to the flow divider).
Through this technique, the three ultrasonic vessel wall
layers (intima media, adventitia, and periadventitia) were
made clearly visible. Technical ultrasound parameters
(dynamic range, depth range, power, reject, edge, gray
scale, and smooth) were kept constant.
The aforementioned ultrasound-based morphological
classification (
Schmidt-Trucksass et al., 1999; Howard
et al., 1993; Belcaro et al., 1996
) included five classes,
with scores ranging 0
e8 (
) for each
artery. In the present study, classes I and II were merged
into a single category, as they could not be univoquely
identified using histological results only.
Table 1
Ultrasound morphology and classes.
Class
Ultrasound Morphology
I
Normal: Three ultrasonic layers (intimae-media,
adventitia, and periadventitia) clearly separated.
No disruption of lumen-intimae interface for
at least 3.0 cm, and/or initial alterations
(lumen-intimae interface disruption at
intervals of
<0.5 mm).
II
Intimae-media granulation: Granular
echogenicity of deep, normally unechoic
intimal-medial layer and/or increased
intimae-media thickness (1 mm).
III
Plaque without haemodynamic disturbance:
Localized wall thickening and increased density
involving all ultrasonic layers. Intimae-media
thickness
>2 mm.
IV
Stenotic plaque: As in III, but with haemodynamic
stenosis on duplex scanning (sample volume
in the centre of the lumen), indicating
stenosis
>50%.
70
F. Cerritelli et al.

A single ultrasound score for each subject was obtained
as the sum of the scores recorded for the four arteries
(
), measured through the aid of VHS.
All characteristics recorded for each individual were
computerized using an Excel spreadsheet by the osteopath,
including results of automated cardiologic measurements
(instrumental print out).
Statistical analysis
Descriptive analysis was performed using frequencies,
arithmetic means and standard deviations. Univariate
statistical tests included formal tests of differences
between study and control groups using
c
2
for categorical
variables and unpaired t tests for continuous measure-
ments. Primary outcomes included differences in pre
epost
changes of IMT, systolic blood pressure (SBP) and diastolic
blood pressure (DBP). Potential confounders included the
following categorical variables: gender, total dose of CA
2
þ
,
ACE, BB and diuretic alone and in combination, OMT.
Continuous variables were categorized to favour clinical
interpretation, based upon upper quartiles: baseline values
of age (
55, >55), BMI (25, >25), heart rate (72, >72),
IMT (
4, >4), SBP (154, >154), DBP (96, >96) and total
daily dose of the above medications (
75 mg, >75).
Multivariate linear regression was used to estimate the
independent effect of OMT on primary outcomes, simulta-
neously adjusting for all other potential confounders, and
pre
epost changes in the endpoints (where relevant).
Statistical significance was based on a probability level
(alpha) equal to 0.05. Results were expressed in terms of
point estimates and 95% confidence intervals (c.i.). All
analyses were performed using the statistical programming
language R (
The R Development Core Team, 2008
).
Results
Association between clinical patterns and primary
outcomes
Descriptive statistical analysis showed no significant
imbalances among treated and control groups in terms of
main characteristics measured at baseline, including phar-
macological treatment (
). Patients were evenly
distributed across classes of B-ultrasound morphology.
At the end of follow-up, all subgroups identified by
different levels of potential confounders, except for
patients not submitted to OMT, showed a general
improvement in all primary endpoints (
). Reduc-
tions observed across all categories ranged between 0.12
and 0.53 mm for IMT, 21.69 and 26.48 mmHg for SBP, and
9.16 and 13.71 mmHg for DBP.
At univariate analysis, baseline characteristics were
found to be significantly associated to the main endpoints
as follows: baseline BMI to change in SBP (p
Z 0.03); heart
rate to change in DBP (p
Z 0.03); SBP to change in IMT
(p
Z 0.04); baseline SBP/DBP to change in DBP (p < 0.01;
<0.001); baseline IMT to change in DBP (p < 0.001); OMT to
change in IMT (p
< 0.0001), SBP (p < 0.0001) and DBP
(p
< 0.01).
The independent role of OMT
Multivariate linear regression (
) showed that in-
creased BMI was significantly associated to a deterioration of
IMT (mean difference per unit between change in treated
and control groups: 0.046; 95% c.i.: 0.004, 0.088), as well as
change in total medications (0.007; 0.001, 0.006), baseline
SBP to lowered SBP (
0.894; 1.239, 0.550) and increased
DBP (0.591; 0.249, 0.933), change in SBP to increased DBP
(0.394; 0.168, 0.621), baseline DBP to increased SBP (0.654;
0.173, 1.135) and decreased DBP (
1.080; 1.422, 0.740),
change in DBP to increased SBP (0.499; 0.212, 0.785).
After adjusting for all the above characteristics, OMT
was found to be significantly and independently associated
to a significant improvement in IMT (
0.517; 0.680,
0.353) and SBP (4.317; 6.421, 2.214), but not to
a difference between changes in DBP.
Discussion
The aim of the present study was to evaluate the efficacy of
OMT on a population of patients affected by essential
hypertension, in terms of improvements in IMT and BP.
To the best of our knowledge, the application of OMT in the
prevention of cardiovascular diseases has never been inves-
tigated in detail, except for observational studies focusing on
BP (
Johnston and Golden, 2001; Johnston and Kelso, 1995;
Kuchera and Kuchera, 1994; Spiegel et al., 2003
).
Our study shows that, after one-year follow-up, OMT is
associated to improved IMT and SBP.
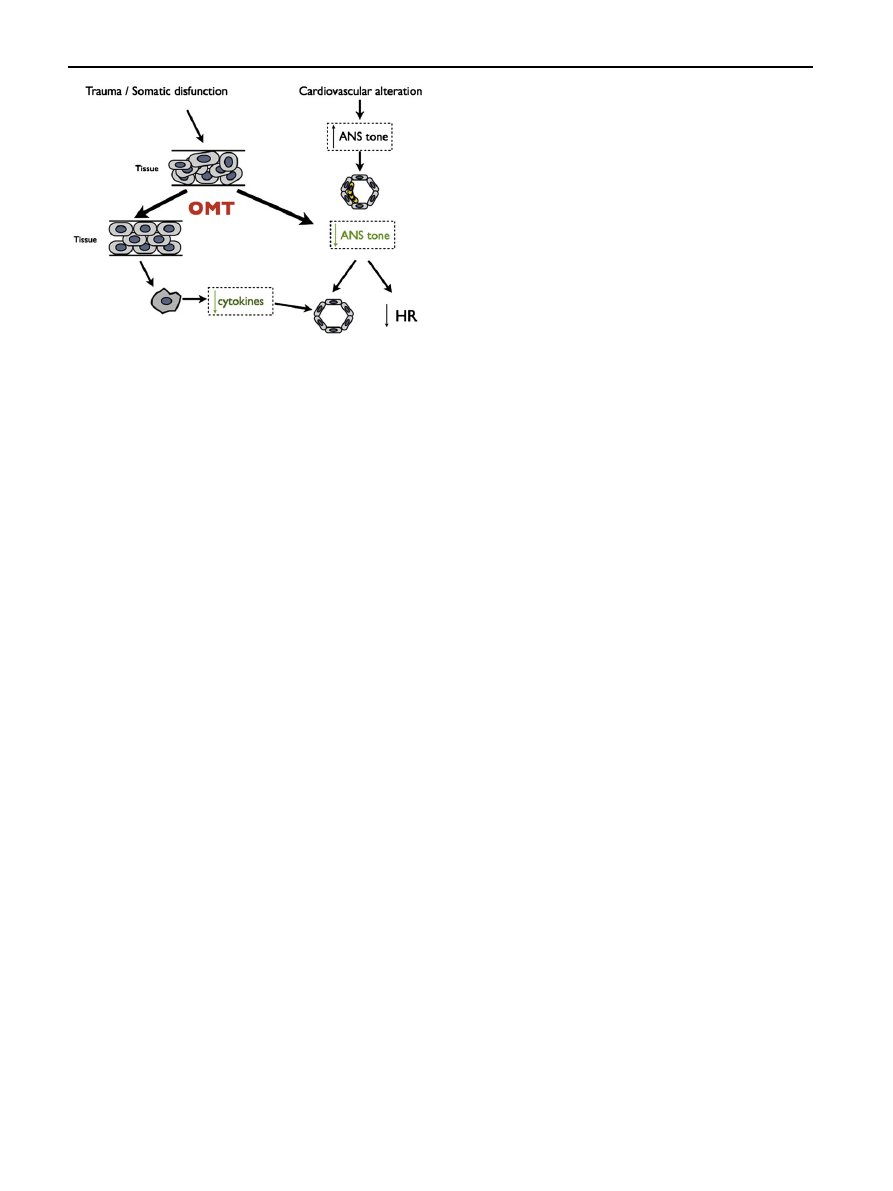
A possible explanatory mechanism is shown in the hypo-
thetical diagram reproduced in
, explained as follows.
In the presence of trauma or somatic dysfunction
changing the structure of the tissue, OMT, consistently with
in-vitro models (
), may decrease
the production of inflammatory factors (cytokines), gener-
ating a cascade effect on mechanisms that generally
Table 2
General characteristics of the study population
at baseline (t
0
).
Study group
Control group
p value
N
31 (49.2)
32 (50.8)
16 (51.6)
15 (46.9)
0.70
Age
50.0
5.7
49.6
6.1
0.79
Height
1.7
0.1
1.7
0.1
0.75
Weight
68.3
8.1
67.9
8.6
0.86
CA
2+
13 (59.1)
9 (40.9)
0.75
ACE
5 (38.4)
8 (61.5)
0.96
15 (46.9)
17 (53.1)
0.47
Diuretics
3 (42.9)
4 (57.1)
0.23
Tot dose
50.1
64.9
51.6
65.1
0.92
IMT
2.8
1.5
3.0
1.6
0.61
BMI
24.2
1.7
24.2
1.3
0.95
SBP
148.9
5.7
149.2
6.1
0.85
DBP
93.4
4.3
93.1
4.0
0.73
Heart rate
69.1
4.0
69.0
4.4
0.97
Numbers in table are mean
s.d.; p value from t test.
* n(%); p value from
c
2
test.
Osteopathic Manipulative Therapy
71
improve the metabolism of the arterial wall. On the other
hand, OMT may also improve the functionality of the
sympathetic nerve system (ANS) affected by a cardiovas-
cular event, re-establishing the physiological function of
the spinal cord (
Johnston and Kelso, 1995; Kuchera and
). Through the important role played by the
sympathetic tone in modifying the metabolism and hemo-
dynamic factors (
), OMT may then
affect the metabolism of the arterial wall, especially in
situations in which the state of intima media is not
substantially compromised (classes II and III).
In our case, all patients showed a general improvement
after 12 months of cardiologic care. The result is consistent
with the effective application of clinical guidelines for the
strict monitoring and control of high risk patients. In this
framework, the results that we obtained through the
application of OMT may represent an important indication
of the possible added value that can be obtained by
introducing a noninvasive complementary treatment in
routine cardiologic practice.
Further investigations, including experimental tests and
randomized clinical trials, are needed to shed light on the
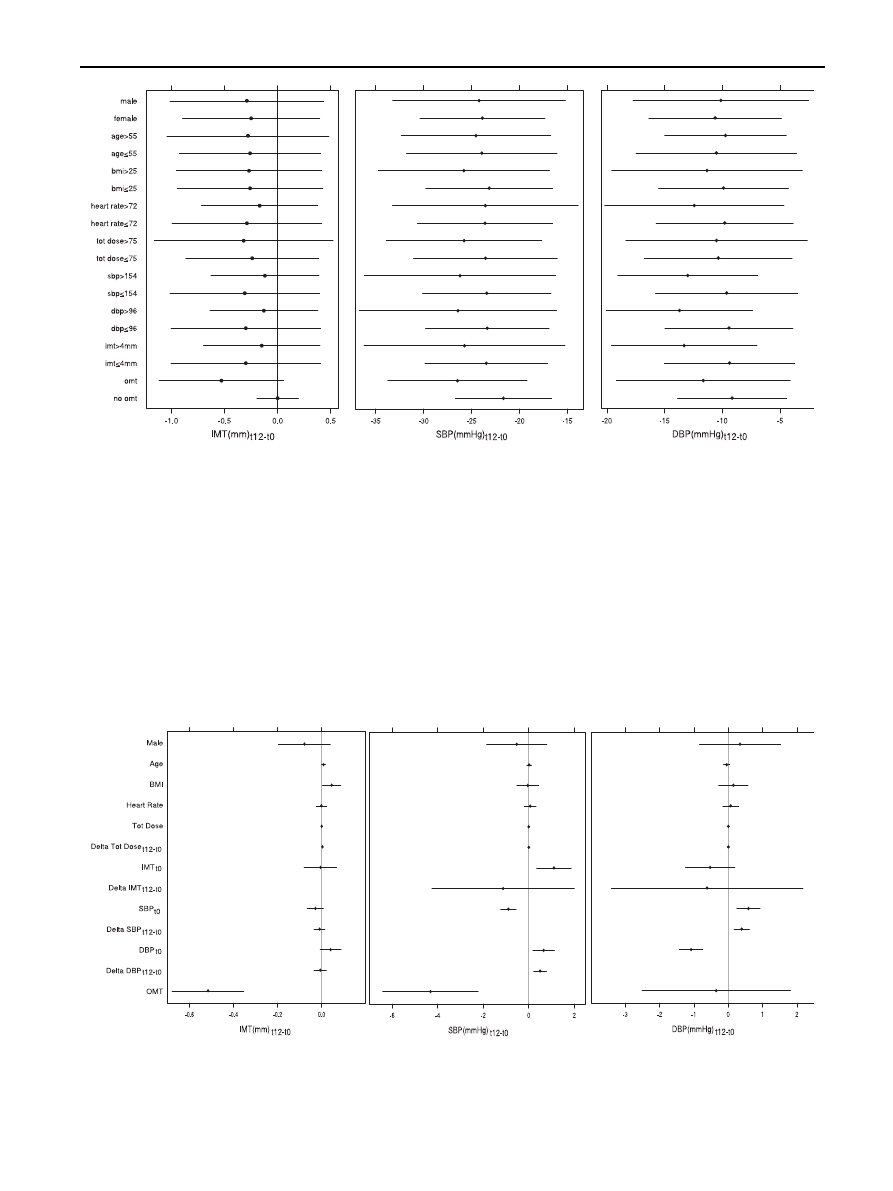
Figure 1
Figure summarizes results from univariate statistical analysis that showed an association between clinical patterns and
primary outcomes at the end of follow-up. Bmi
Z body mass index, sbp Z systolic blood pressure, dbp Z diastolic blood pressure,
imt
Z intima media thickness, omt Z osteopathic manipulative treatment.
Figure 2
Figure describes results from multivariate linear regression that showed an independent role of OMT on primary
outcomes. BMI
Z body mass index, IMT Z intima media thickness, SBP Z systolic blood pressure, DBP Z diastolic blood pressure,
OMT
Z osteopathic manipulative treatment.
72
F. Cerritelli et al.
actual mechanisms involved in the application of OMT on
cardiovascular parameters.
To overcome the scarcity of information available in this
field, new studies should also incorporate methodological
procedures that were not applied in our case purely for
practical reasons. In particular treatment was not randomly
assigned, the sample size was not based on a formal power
computation, and the sample treated by a single cardiolo-
gist/osteopath may not represent adequately the average
target population.
Nevertheless, the present study shows that after a one-
year follow-up, osteopathic treatment is associated to
improved conditions of the arterial wall and reduced blood
pressure. These results highlight a potential beneficial
effect of osteopathic manipulation in the management of
subjects at high risk of cardiovascular events, using
measures that can be easily obtained in similar conditions
in everyday cardiologic practice at the international level.
Our approach, mainly exploratory and hypothesis
generating, may be used as a basis for further investigation
in different populations and practices.
The strength and causal explanations of the efficacy of
osteopathic treatment on key clinical parameters need to
be validated under more general conditions.
Disclosure
None.
Appendix A
Supplementary data
Supplementary data associated with this article can be
found, in the online version, at
References
Belcaro, G., Nicolaides, A.N., Laurora, G., Cesarone, M.R., De
Sanctis, M., Incandela, L., et al., 1996. Ultrasound morphology
classification of the arterial wall and cardiovascular events in
a 6-year follow-up study. Arteriosclerosis Thrombosis and
Vascular Biology 16, 851
e856.
Belcaro, G., Nicolaides, A.N., Ramaswami, G., Cesarone, M.R., De
Sanctis, M., Incandela, L., et al., 2001. Carotid and femoral
ultrasound morphology screening and cardiovascular events in
low risk subjects: a 10-year follow-up study (the CAFES-CAVE
study(1)). Atherosclerosis 156, 379
e387.
Brookes, L., 2004. The updated WHO/ISH hypertension guidelines.
Medscape Cardiology Available at:
.
Carter, J.B., Banister, E.W., Blaber, A.P., 2003. Effect of endurance
exercise on autonomic control of heart rate. Sports Medicine
33, 33
e46.
Charkoudian, N., Joyner, M.J., Johnson, C.P., Eisenach, J.H.,
Dietz, N.M., Wallin, B.G., 2005. Balance between cardiac output
and sympathetic nerve activity in resting humans: role in arterial
pressure regulation. Journal of Physiology 568, 315
e321.
Cheitlin, M.D., 2003. Cardiovascular physiology-changes with aging.
American Journal of Geriatric Cardiology 12, 9
e13.
Cheng, K.S., Mikhailidis, D.P., Hamilton, G., Seifalian, A.M., 2002.
A review of the carotid and femoral intima-media thickness as
an indicator of the presence of peripheral vascular disease and
cardiovascular
risk
factors.
Cardiovascular
Research
54,
528
e538.
Dinenno, F.A., Jones, P.P., Seals, D.R., Tanaka, H., 2000. Age-
associated arterial wall thickening is related to elevations in
sympathetic activity in healthy humans. American Journal of
Physiology,
Heart
and
Circulatory
Physiology
278,
H1205
eH1210.
Goldsmith, R.L., Bloomfield, D.M., Rosenwinkel, E.T., 2000. Exer-
cise and autonomic function. Coronary Artery Disease 11,
129
e135.
Greenman, P.E., 2003. Principles of Manual Medicine, third ed.
Lippincott Williams & Wilkins, Philadelphia.
Howard,
G.,
Sharrett,
A.R.,
Heiss,
G.,
Evans,
G.W.,
Chambless, L.E., Riley, W.A., et al., 1993. Carotid artery
intimal-medial thickness distribution in general populations as
evaluated by B-mode ultrasound. ARIC Investigators. Stroke
24, 1297
e1304.
Johnston, W.L., Golden, W.J., 2001. Segmental definition
epart IV.
Updating the differential for somatic and visceral inputs.
Journal of American Osteopathic Association 101, 278
e283.
Johnston, W.L., Kelso, A.F., Babcock, H.B., 1995. Changes in
presence of a segmental dysfunction pattern associated with
hypertension: part 1. A short-term longitudinal study. Journal of
American Osteopathic Association 95, 243
e248. 253e255.
Johnston, W.L., Kelso, A.F., 1995. Changes in presence of
a segmental dysfunction pattern associated with hypertension:
part 2. A long-term longitudinal study. Journal of American
Osteopathic Association 95, 315
e318.
Kalinina, O.V., Efimova, E.G., 2006. Effects of different methods of
physical therapy on the course of autonomic dysfunction
syndrome. Voprosy Kurortologii, Fizioterapii, I Lechebno
ĭ Fizi-
chesko
ĭ Kultury 1, 19e21.
Kuchera, W.A., Kuchera, M.L., 1994. Osteopathic Principles in
Practise. Greyden Press, Columbus.
Labropoulos, N., Ashraf Mansour, M., Kang, S.S., Oh, D.S.,
Buckman, J., Baker, W.H., 2000. Viscoelastic properties of
normal and atherosclerotic carotid arteries. European Journal
of Vascular and Endovascular Surgery 19, 221
e225.
Longmire, D.R., 2006. An electrophysiological approach to the
evaluation of regional sympathetic dysfunction: a proposed
classification. Pain Physician 9, 69
e82.
Meltzer, K.R., Standley, P.R., 2007. Modeled repetitive motion strain
and indirect osteopathic manipulative techniques in regulation of
human fibroblast proliferation and interleukin secretion. Journal
of American Osteopathic Association 107, 527
e536.
Figure 3
Hypothetical diagram shows a possible explanatory
mechanisms of OMT based on cardiovascular and neurological
patterns. ANS
Z autonomic nervous system, HR Z heart rate.
Osteopathic Manipulative Therapy
73

Narkiewicz,
K.,
Phillips,
B.G.,
Kato,
M.,
Hering,
D.,
Bieniaszewski, L., Somers, V.K., 2005. Gender-selective inter-
action between aging, blood pressure, and sympathetic nerve
activity. Hypertension 45, 522
e525.
Rosenwinkel, E.T., Bloomfield, D.M., Arwady, M.A., Goldsmith, R.L.,
2001. Exercise and autonomic function in health and cardiovas-
cular disease. Cardiology Clinics 19, 369
e387.
Safar, M.E., Levy, B.I., Struijker-Boudier, H., 2003. Current
perspectives on arterial stiffness and pulse pressure in hyper-
tension and cardiovascular diseases. Circulation 107, 2864
e2869.
Schmidt-Trucksass, A., Grathwohl, D., Schmid, A., Boragk, R.,
Upmeier, C., Keul, J., et al., 1999. Structural, functional, and
hemodynamic changes of the common carotid artery with age in
male subjects. Arteriosclerosis Thrombosis and Vascular Biology
19, 1091
e1097.
Simon, A., Gariepy, J., Chironi, G., Megnien, J.L., Levenson, J., 2002.
Intima-media thickness: a new tool for diagnosis and treatment of
cardiovascular risk. Journal of Hypertension 20, 159
e169.
Spiegel, A.J., Capobianco, J.D., Kruger, A., Spinner, W.D., 2003.
Osteopathic manipulative medicine in the treatment of hyper-
tension: an alternative, conventional approach. Heart Disease
5, 272
e278.
Tanaka, H., Seals, R.D., Monahan, K.D., Clevenger, C.M.,
DeSouza, C.A., Dinenno, F.A., 2002. Regular aerobic exercise
and the age-related increase in carotid artery intima-media
thickness in healthy men. Journal of Applied Physiology 92,
1458
e1464.
The R Development Core Team, 25 August 2008. R: a language and
environment for statistical computing. Available at:
r-project.org/doc/manuals/fullrefman.pdf
Reference index,
version 2.7.2.
Williams, A.M., 1994. An osteopathic cardiologist’s review of
hypertension: beyond the Fifth Report of the Joint National
Committee on Detection, Evaluation, and Treatment of High
Blood Pressure. Journal of American Osteopathic Association
94, 833
e847.
74
F. Cerritelli et al.
Document Outline
- Osteopathic manipulation as a complementary treatment for the prevention of cardiac complications: 12-Months follow-up of i ...
Wyszukiwarka
Podobne podstrony:
Osteopathic manipulative treatm Nieznany
Osteopathic manipulative treatment 1
FIZJOTERAPIA w osteoporozie
osteoporoza 3
Otyłość a osteoporoza
Osteoporaza diag i lecz podsumow interna 2008
9 Osteoporoza
osteoporoza 7
Osteoporosis ľ diagnosis and treatment
Rodzaje manipulacji
Fizjoterapia w osteoporozie
Patomechanizmy zaburzeń gospodarki wapniowo fosforanowej; osteoporoza
SEM[1] 05 Zapalenia kosci i osteoporoza
DIAGNOSTYKA, PROFILAKTYKA I LECZENIE OSTEOPOROZY 2
04 Analiza kinematyczna manipulatorów robotów metodą macierz
osteoporoza i dna
Genetyczne manipulacje inżynierska katastrofa
więcej podobnych podstron