
CHAPTER 12
Principles of Neurosurgery,
edited by Robert G. Grossman. Rosenberg © 1991.
Published by Raven Press, Ltd., New York.
Head Injury
Raj K. Narayan
Causes, 236
Classification, 236
By Mechanism, 237
By Severity, 237
By Morphology, 237
Management of Head Injury, 239
Mild Head Injury, 239
Moderate Head Injury, 240
Severe Head Injury, 241
Surgical Considerations, 258
Anesthesia, 258
Subdural Hematomas, 258
Epidural Hematomas, 258
Intracerebral Hematomas, 259
Posterior Fossa Hematomas, 260
Depressed Fractures, 261
Penetrating Head Injuries, 261
Venous Sinus Injuries, 262
Therapeutic Agents, 262
Anticonvulsants, 262
Steroids, 264
Mannitol, 264
Lasix, 265
Sodium Bicarbonate, 265
Tris-hydroxy-methyl-aminomethane (THAM), 265
Barbiturates, 265
Naloxone, 266
Short-Acting Hypnotics, 266
Hyperbaric Oxygen, 266
Free Radical Scavengers, 266
Intracranial Pressure Monitoring and Control, 266
Basic Physiology, 266
Technical Aspects, 268
Value of ICP Monitoring, 268
Indications for ICP Monitoring, 269
Treating Raised ICP, 269
Complications of ICP Monitoring, 270
Management of Associated Injuries, 270
Scalp Injuries, 270
Maxillofacial Injuries, 271
Injuries of the Spine, 273
Orthopedic Injuries, 275
Chest Injuries, 275
Vascular Injuries, 277
Abdominal Injuries, 277
Renal Injuries, 277
Ophthalmological Injuries, 278
Sequelae of Head Injury, 278
Cranial Nerve Injuries, 279
Locked-in Syndrome, 280
Peripheral Neuropathies, 280
Posttraumatic Hydrocephalus, 281
Cerebrospinal Fluid Fistulas, 282
Posttraumatic Vascular Complications, 283
Prognosis, 285
Conclusion, 285
References, 286
Trauma is the leading cause of death in the United States
for persons between 1 and 44 years of age and is the third
most common cause overall (1). In over half of trauma-
related deaths, head injury contributed significantly to
the outcome (2). In patients with multiple injuries, the
head is the most commonly injured part, and in fatal
road accidents, injury to the brain is found in nearly 75
R. K. Narayan: Department of Neurosurgery, Baylor Col-
lege of Medicine, Houston, Texas 77030.
percent of the victims at autopsy (3). In 1982 there were
approximately 165,000 deaths from trauma in the
United States, and for each death there were at least two
cases of permanent disability, usually secondary to head
injury (4). Trauma accounts for the loss of more poten-
tial work-life years (3.5 million) than cancer (1.8 million)
and cardiovascular disease (1.6 million) combined (5,6).
Because trauma often affects people early in life, its cost
measured in death and disability is very high. The total
annual cost of accidental trauma, including lost wages,
235

236 / CHAPTER 12
medical expenses, and indirect work losses, is estimated
at $75 to 100 billion (7). During the past decade, the
death rates from heart disease and stroke have fallen by
22 percent and 32 percent, respectively, but the death
rate from trauma has risen by approximately 1 percent
each year since 1977 (4).
The incidence of traumatic brain injury in the United
States is conservatively estimated to be approximately
200/100,000 (2). With a total population of 235 million
(1984), this translates into approximately 470.000 new
cases per year (2). Of these, 70.000 patients die before
reaching the hospital. The remaining 400,000 are admit-
ted to hospitals. Of these. 80 percent (320,000) are catego-
rized as mild, 10 percent (40.000) as moderate, and 10
percent (40,000) as severe brain injuries. These figures
do not include the large number of patients with mild
head injuries who are not admitted to a hospital. It is
estimated that the death rates in the mild, moderate, and
severe categories are 0 percent, 7 percent, and 58 per-
cent, respectively, yielding a total annual mortality of
26.000 patients. Together with the prehospital mortality,
head injury thus accounts for approximately 96,000
deaths per year in the United States (2).
Perhaps even more dramatic than the mortality fig-
ures is the magnitude of the population with residual
disabilities. Again, conservatively, with estimations of a
permanent disability rate of 10 percent in the mild, 66
percent in the moderate, and 100 percent in the severely
brain-injured groups, it is calculated that there are
73,724 new patients with long-term residual disabilities
secondary to brain injury being added to the pool each
year. This includes about 2,000 who remain in a perma-
nent vegetative state (8). The total direct and indirect
cost to the nation for persons with disabilities owing to
brain injury is estimated to be around $25 billion per
year and is increasing.
These figures leave no doubt that death and disability
from trauma in general, and head injury in particular, is
a major public health problem in the United States. Any
therapeutic measures that could reduce the mortality
and morbidity associated with these injuries even
slightly could translate into very significant benefits in
both human and economic terms.
CAUSES
Head injury is primarily an affliction of young adults
between 15 and 44 years of age (9). The average age re-
ported in several series is around 30 years. Males are
affected more than twice as often as females. There does
not appear to be any difference in incidence between
whites and nonwhites in the United States.
Motor vehicle accidents are the most frequent cause of
head injury, accounting for about 49 percent of all cases.
Motor vehicle accidents are associated with more severe
head injuries and occur more often in those 15 to 24
years of age, whereas falls occur more often in the pediat-
ric age group and usually result in less severe injuries.
Patients involved in motor vehicle accidents often sus-
tain multiple injuries. In one series of severely head-in-
jured patients, more than 50 percent were found to have
additional major systemic injuries (10). Although the
overall incidence of intracranial hematomas following
head injury is only 2 percent, approximately one-half of
the patients who arrive at the hospital unconscious from
a head injury will have a major intracranial hema-
toma (11).
For head injury there is an early peak in occurrence in
April, followed by a general increase to the highest
monthly percentage in September (9). Most head and
spinal cord injuries occur on Fridays, Saturdays, and
Sundays, times when coverage in hospitals is often less
than optimal. Thus, we are dealing with a very common
problem that tends to occur at inconvenient times, de-
mands a lot of time and attention, and can lead to disas-
trous results if not handled rapidly and appropriately.
Although a great deal has been learned about central
nervous system trauma, both at a cellular and at a clini-
cal level, much remains controversial. In the following
account we have outlined our approach, trying to indi-
cate controversial aspects whenever they appear. How-
ever, it must be emphasized that the management proto-
cols described here are not entirely based on
incontrovertible scientific data. They are certainly not
the only correct way of managing head injury.
CLASSIFICATION
Head injuries may be classified in several ways. For
practical purposes, three means of classification are use-
ful—classification by mechanism, severity, and morphol-
ogy (Table 1).
_____TABLE 1. Classification of head injury______
A. By mechanism
1 . Closed
2. Penetrating
B. By severity
1 . Glasgow Coma Scale score
2. Mild, moderate, severe
C. By morphology
1 . Skull fractures
a. Vault
(1) Linear or stellate
(2) Depressed or nondepressed
b. Basilar
2. Intracranial lesions
a. Focal
(1) Epidural
(2) Subdural
(3) Intracerebral
(1) Mild concussion
(2) Classical concussion
(3) Diffuse axonal injury

HEAD INJURY / 237
By Mechanism
Head injury may be broadly classified as closed or
penetrating. Although these terms are widely used and
are useful from a descriptive point of view, they are not
mutually exclusive. For example, a depresse skull frac-
ture could be variably assigned to either one of these two
categories, depending on the depth and severity of the
bony injury. Nevertheless, for practical purposes, the
term "closed head injury" is usually associated with auto
accidents, falls, and assaults, and "penetrating head in-
jury" is most often associated with gunshot wounds and
stab injuries. Because the management of these two
broad groups is slightly different, we shall maintain this
distinction for descriptive purposes.
By Severity
Prior to 1974, different authors used terminology with
variable connotations to describe patients with head in-
jury, making it virtually impossible to compare groups of
patients from different centers. In 1974 Teasdale and
Jennett, by studying the signs that seemed to predict out-
come most reliably and which seemed to have the least
interobservcr variation, designed what has come to be
known as the Glasgow Coma Scale (GCS). The introduc-
tion of the GCS (Table 2) brought some degree of unifor-
mity and discipline into the head injury literature (12).
This scale has achieved widespread use for the descrip-
tion of patients with head injury and, furthermore, has
been adopted for the description of patients with altered
levels of consciousness from other causes.
Jennett and Teasdale defined coma as the inability to
obey commands, utter words, or open the eyes (13). The
patient who does not meet all three aspects of this defini-
tion is not considered comatose. In a series with 2,000
TABLE 2. The Glasgow Coma Scale (GCS)
a
Eye opening (E)
Spontaneous
To call
To pain
None
Motor response (M)
Obeys commands
Localizes pain
Normal flexion (withdrawal)
Abnormal flexion (decorticate)
Extension (decerebrate)
None (flaccid)
Verbal response (V)
Oriented
Confused conversation
Inappropriate words
Incomprehensible sounds
None
4
3
2
1
6
5
4
3
2
1
5
4
3
2
1
a
GCS sum score = (E + M + V); best possible score = 1 5 ;
worst possible score = 3
patients with a severe head injury, these authors ob-
served 4 percent who did not speak but obeyed com-
mands and another 4 percent who uttered words but did
not obey. Among patients who could neither obey nor
speak, 16 percent opened their eyes and were therefore
judged not to be in coma. Patients who open their eyes
spontaneously, obey commands, and are oriented score
a total of 15 points, whereas flaccid patients who do not
open their eyes or talk score the minimum of 3 points.
No single score within the range of 3 to 15 forms the
cut-off point for coma. However, 90 percent of all pa-
tients with a sum score of eight or less, and none of those
with a score of nine or more, are found to be in coma
according to the preceding definition. For all practical
purposes, a GCS sum score of eight or less has become
the generally accepted definition of a comatose patient.
The distinction between patients with severe head injury
and those with mild to moderate injury is thus fairly
clear. However, distinguishing between mild and moder-
ate head injury is more of a problem (14). Somewhat
arbitrarily, head-injured patients with a GCS sum score
of 9 to 12 have been categorized as moderate, and those
with a GCS score of 13 to 15 have been designated mild.
Williams, Levin, and Eisenberg have recently reported
that neurobehavioral deficits in patients with mild head
injury (GCS 12 to 15) with an intracranial lesion on ini-
tial computed tomography (CT) were similar to those in
patients with moderate head injury (GCS 9 to 11). Pa-
tients with mild head injury uncomplicated by an intra-
cranial lesion on CT scan did significantly better (15).
By Morphology
The advent of CT scanning has revolutionized the clas-
sification and management of head injury. Thus, al-
though certain patients who are rapidly deteriorating
may be taken to surgery without a CT scan, the vast
majority of severely injured patients should have the
benefit of a CT scan prior to surgical intervention. Fur-
thermore, frequent follow-up CT scans are essential be-
cause the morphological picture in head injury often un-
dergoes a remarkable evolution over the first few hours,
days, and even weeks after the injury. Morphologically,
head injuries may be broadly considered under two head-
ings: skull fractures and intracranial lesions.
Skull Fractures
Skull fractures may be seen in the cranial vault or skull
base, may be linear or stellate, and may be depressed or
nondepressed. Basal skull fractures are harder to docu-
ment on plain x-rays and usually require CT scanning
with bone-window settings to demonstrate their loca-
tion. The presence of clinical signs of a basal skull frac-
ture should increase the index of suspicion and help in
their identification. As a general guideline, fragments de-

238 / CHAPTER 12
pressed more than the thickness of the skull require ele-
vation. Open or compound skull fractures have a direct
communication between a scalp laceration and the cere-
bral surface because the dura is torn, and these fractures
require early surgical repair.
To quote Jennett and Teasdale, "To the lay mind, and
particularly to the legal mind, fracture of the skull is an
obvious mark of severity following a head injury. Thou-
sands of heads are x-rayed in emergency rooms, but in
only two or three cases in a hundred is there a fracture;
consequently, radiologists write papers on the misuse of
resources and demand that clinicians do better triage be-
fore x-rays are done. Neurosurgeons have long preached
that assessment of the conscious level is more important
than a skull x-ray, and this has been mistakenly taken to
imply that they regard the detection of a fracture as un-
important, especially after milder injuries. In fact, it is in
the patient whose consciousness is unimpaired and who
might otherwise be sent home as a trivial injury that
finding a fracture can be most significant, because it
alerts the clinician to the risk of complications such as
intracranial hematoma or infection" (16). The fre-
quency of skull fractures varies, with more fractures be-
ing found if the population studied has greater prepon-
derance of severe injuries. A linear vault fracture
increases the risk of intracranial hematoma by about 400
times in a conscious patient and by 20 times in a coma-
tose patient. For this reason, the detection of a skull frac-
ture warrants admission to hospital for observation, no
matter how well the patient seems.
Intracranial Lesions
These may be classified as focal or diffuse, although
these two forms of injury frequently coexist. Focal le-
sions include epidural hematomas, subdural hemato-
mas, and contusions (or intracerebral hematomas). Pa-
tients in the diffuse brain injury group, in general, have
normal CT scans but demonstrate an altered sensorium
or even deep coma. The cellular basis of diffuse brain
injury has become much clearer in recent years.
Focal Lesions
Epidural Hematomas. These clots are located outside
the dura but within the skull. They are most often lo-
cated in the temporal or temporal-parietal region and are
often due to tearing of the middle meningeal vessels.
These clots are usually thought to be arterial in origin,
but they may be secondary to venous bleeding in at least
one-third of cases. Occasionally, an epidural hematoma
may result from torn venous sinuses, particularly in the
parietal-occipital region or posterior fossa. Although epi-
dural hematomas are relatively uncommon (0.5 percent
of all and 9 percent of comatose head-injured patients),
they should always be considered in the diagnostic pro-
cess and treated rapidly. If treated early, the prognosis is
usually excellent because the underlying brain injury is
usually limited. Outcome is directly related to the status
of the patient before surgery. The mortality from epidu-
ral hematoma approximates 0 percent for patients not in
coma, 9 percent for obtunded patients, and 20 percent
for patients in deep coma.
Subdural Hematomas. These are much more com-
mon than epidural hematomas, being found in approxi-
mately 30 percent of patients with severe head injuries.
They occur most frequently from a tearing of bridging
veins between the cerebral cortex and the draining si-
nuses. However, they can also be associated with lacera-
tions of the brain surface or substance. A skull fracture
may or may not be present. Furthermore, the brain dam-
age underlying acute subdural hematomas is usually
much more severe and the prognosis much worse than
for epidural hematomas. The mortality in a general se-
ries may be around 60 percent, but it may be lowered by
very rapid surgical intervention and aggressive medical
management (17).
Contusions and Intracerebral Hematomas. Pure cere-
bral contusions are a fairly common occurrence. Their
frequency has become much more apparent as the qual-
ity and number of CT scanners have increased. Further-
more, contusions of the brain are almost always seen in
association with subdural hematomas. The vast majority
of contusions occur in the frontal and temporal lobes,
although they can occur at almost any site including the
cerebellum and brainstem. The distinction between con-
tusions and traumatic intracerebral hematomas remains
somewhat ill-defined. The classical "salt-and-pepper"
type of lesion is clearly a contusion, and a large hema-
toma is clearly not. However, there is a gray zone, and
contusions can evolve into intracerebral hematomas
over a period of hours or days.
Diffuse Injuries
Diffuse brain injuries form a continuum of progres-
sively severe brain damage that is caused by increasing
amounts of acceleration-deceleration injury to the brain.
In its pure form, diffuse brain injury is the most com-
mon type of head injury.
Mild Concussion. Mild concussion is that injury in
which consciousness is preserved but there is some de-
gree of noticeable temporary neurological dysfunction.
These injuries are exceedingly common and, because of
their mild degree, are often not brought to medical atten-
tion (18). The mildest form of concussion results in con-
fusion and disorientation without amnesia. This syn-
drome is usually completely reversible and is associated
with no major sequelae. Slightly more severe head injury
causes confusion with both retrograde and posttrau-
matic amnesia.
HEAD INJURY / 239
Classical Cerebral Concussions. Classical cerebral
concussion is the posttraumatic state that results in loss
of consciousness. This condition is always accompanied
by some degree of retrograde and posttraumatic amne-
sia, and the length of posttraumatic amnesia is a good
measure of the severity of the injury. The loss of con-
sciousness is transient and reversible. As a somewhat ar-
bitrary definition, the patient has returned to full con-
sciousness by six hours, although it is usually much
sooner. The great majority of patients with classical cere-
bral concussion have no sequelae other than amnesia for
the events relating to the injury, but some patients may
have more long-lasting, although sometimes subtle, neu-
rological deficits.
Diffuse Axonal Injury. Diffuse axonal injury (DAI) is
the term used to describe prolonged posttraumatic coma
that is not due to mass lesions or ischemic insults. Loss of
consciousness from the time of injury continues beyond
six hours. This phenomenon may be further broken
down into mild, moderate, and severe categories. Mild
DAI is relatively uncommon and is defined as that group
in which coma lasts from 6 to 24 hours, with patients
starting to follow commands by 24 hours. Moderate DAI
is defined as coma lasting more than 24 hours without
prominent brainstem signs. This is the most common
form of DAI and comprises 45 percent of all patients
with DAI. Severe DAI usually occurs in vehicular acci-
dents and is the most devastating form. It comprises
about 36 percent of all patients with DAI. These patients,
are rendered deeply comatose and remain so for pro-
longed periods of time. They often demonstrate evi-
dence of decortication or decerebration and often re-
main severely disabled, if they survive. These patients
often exhibit autonomic dysfunction such as hyperten-
sion, hyperhidrosis, and hyperpyrexia and were
previously designated as having primary brainstem in-
jury. It is now believed that diffuse axonal injury is the
much more common physiological basis for this clinical
picture (18).
MANAGEMENT OF HEAD INJURY
Mild Head Injury
The vast majority of patients presenting to the emer-
gency room with head injuries fall under this category
(Fig. 1). These patients are awake when seen by the phy-
sician but may be amnesic for events surrounding the
injury. There may be a history of a briefless of conscious-
ness, which is usually difficult to confirm. The issue
is often further confounded by alcohol or other intoxi-
cants (19).
DEFINITION: The patient is awake, and may be oriented.
MANAGEMENT:
1 . History: Type and time of accident, loss of consciousness,
amnesia, headache
2. General examination to rule out systemic injuries
3. Neurological examination
4. Skull radiographs
5. Cervical spine and other radiographs as indicated
6. Blood alcohol level and urine for toxic screen
7. CT scan should ideally be obtained if first seven criteria for
admission noted below are present
CRITERIA FOR ADMISSION
1 . Significant posttraumatic amnesia (over 1 hr)
2. History of loss of consciousness (over 1 5 mins)
3. Deteriorating level of consciousness
4. Moderate to severe headache
5. Intoxication with alcohol or drugs
6. Skull fracture
7. CSF leak - otorrhea or rhinorrhea
8. Significant associated injuries
9. No reliable companion at home
10. Abnormal CTscan
DISCHARGE FROM ER:
1 . If patient does not meet any of the
criteria for admission.
2. Discuss need to return if any problems
develop and issue a "warning sheet."
3. Schedule follow-up clinic visit
within 1 week.
FIG. 1. Management of mild head injury.

240 / CHAPTER 12
Most patients with mild head injury go on to make
uneventful recoveries, albeit with subtle neurological se-
quelae (20). However, about 3 percent of patients unex-
pectedly deteriorate and can become neurologically de-
vastated if the decline in their mental status is not
noticed early (21). How far must a physician go to insure
against such an occurrence? The classical struggle be-
tween "cost-effectiveness" and the "best possible" ther-
apy is clearly evident in this instance. Although practice
in different centers varies (22), we believe the following
measures to be optimal for patients presenting with a
mild head injury.
Skull x-rays may be obtained looking for the following
features: linear or depressed skull fractures, position of
the pineal gland if calcined, air-fluid levels in the sinuses,
pneumocephalus, facial fractures, and foreign bodies.
The routine ordering of skull x-rays in patients with
minor head injury has come under some criticism, and a
multicenter study sponsored by the FDA has recom-
mended guidelines for reducing the number of low-yield
studies (23). Based on an analysis of 7,035 head-injured
patients at 31 hospitals, the panel outlined a strategy
based on the level of risk:
1. For the low-risk group, with minimal initial signs and
symptoms such as headache, dizziness, or scalp lacera-
tions, discharge to a reliable environment for obser-
vation is recommended, with no need for skull radiog-
raphy.
2. For the moderate-risk group, with initial signs such as
vomiting, alcohol and drug intoxication, posttrauma-
tic amnesia, or signs of a basilar or depressed fracture,
the recommended procedure includes extended close
observation, consideration of CT or plain film radiog-
raphy, and a possible neurological consultation.
3. And for the high-risk group, with the most serious
initial symptoms such as depressed or decreasing level
of consciousness, focal neurological signs or penetrat-
ing injuries, a neurological consultation alone or
combined with an emergency CT scan is recom-
mended.
In this study, approximately 75 percent of the 7,035
patients would have been assigned to the low-risk group,
23 percent to the moderate-risk group, and 2 percent to
the high-risk group. Thus, using the panel's strategy,
about three-fourths of the patients with head injuries
would not have required skull x-rays. The panel stressed
that these guidelines were not meant to supplant a clini-
cian's judgment. Furthermore, the severity of injuries
commonly encountered will certainly vary from one hos-
pital to the next.
How often does one find a skull fracture? This figure
varies with the severity of injury from 3 percent of pa-
tients seen in the emergency room with a mild head in-
jury (those not admitted) to 65 percent among those with
severe head injuries (16). The vault is involved three
times as often as the base. It should be remembered,
however, that basal fractures are often not visualized on
initial skull films. Clinical signs of a fractured base—or-
bital hematoma, cerebrospinal fluid (CSF) rhinorrhea or
otorrhea, hemotympanum, or Battle's sign—must be
taken as presumptive evidence of a basal fracture and
warrant admission for observation.
Ideally, a CT scan should be obtained in all patients,
although this is practically and financially impossible in
most institutions at the present time. If the patient is
fully awake and alert and can be kept under observation
for about 12 to 24 hours, this study may be deferred or
even cancelled. Our recommendations relating to the
timing of the CT scan in mild head injury patients re-
main tentative. Although unlikely, it is possible for pa-
tients with normal early scans to develop mass lesions a
few hours later. Close neurological observation by per-
sonnel sensitized to the possibility of deterioration is
without doubt the best safeguard against such "freak"
occurrences.
The cervical spine and other parts must be x-rayed
whenever there is any pain or tenderness. No drugs are
recommended except non-narcotic analgesics such as
Tylenol. Tetanus toxoid must be administered if there
are any associated open wounds. Routine blood tests are
usually not necessary if there are no systemic injuries. A
blood-alcohol level and urine toxic screen may be indi-
cated for m^dicolegal purposes.
Our practice with a mildly head-injured patient with a
normal CT scan is to discharge her or him to the care of a
reliable companion, who is instructed according to a
"warning sheet" (Fig. 2) to keep the patient under close
observation for at least 12 hours and to bring the patient
back if any adverse features develop. If no reliable com-
panion is available, the patient is kept in the emergency
room holding area for 12 hours with neurological checks
every half-hour and is then discharged if he or she ap-
pears stable.
If a lesion is noted on CT scan, the patient must be
admitted and managed according to his or her neurologi-
cal progress over the next few days. A follow-up CT scan
is usually obtained prior to discharge, or sooner in the
case of neurological deterioration. The management of
head injuries in athletes has been reviewed elsewhere
(24,25).
Moderate Head Injury
Although these patients are still able to follow simple
commands, they can deteriorate rapidly (26). Therefore,
they should be treated in a manner akin to the severely
head-injured patient, although perhaps with a less acute
sense of urgency (Fig. 3). Several authors have detailed
their experience with this category of patients (27).
On admission to the emergency room, a brief history
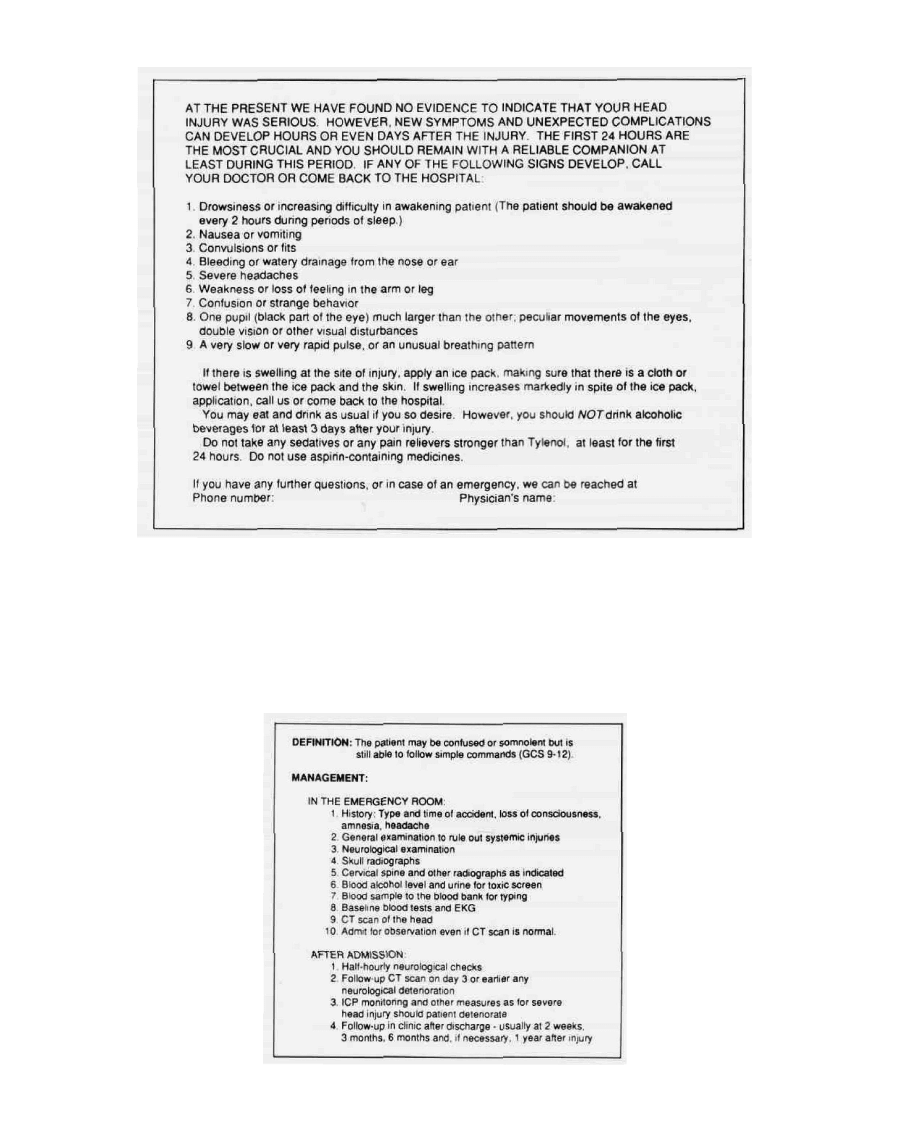
HEAD INJURY / 241
FIG. 2. Warning sheet for patients with mild head injury who are to be sent home.
is obtained and cardiopulmonary stability ensured prior
to neurological assessment. Blood work may include a
CBC, SMA 20, coagulation profile, alcohol level, and a
sample for the blood bank. Cervical spine films are ob-
tained, and a CT scan is generally indicated. The pa-
tient is admitted for observation even if the CT scan is
normal.
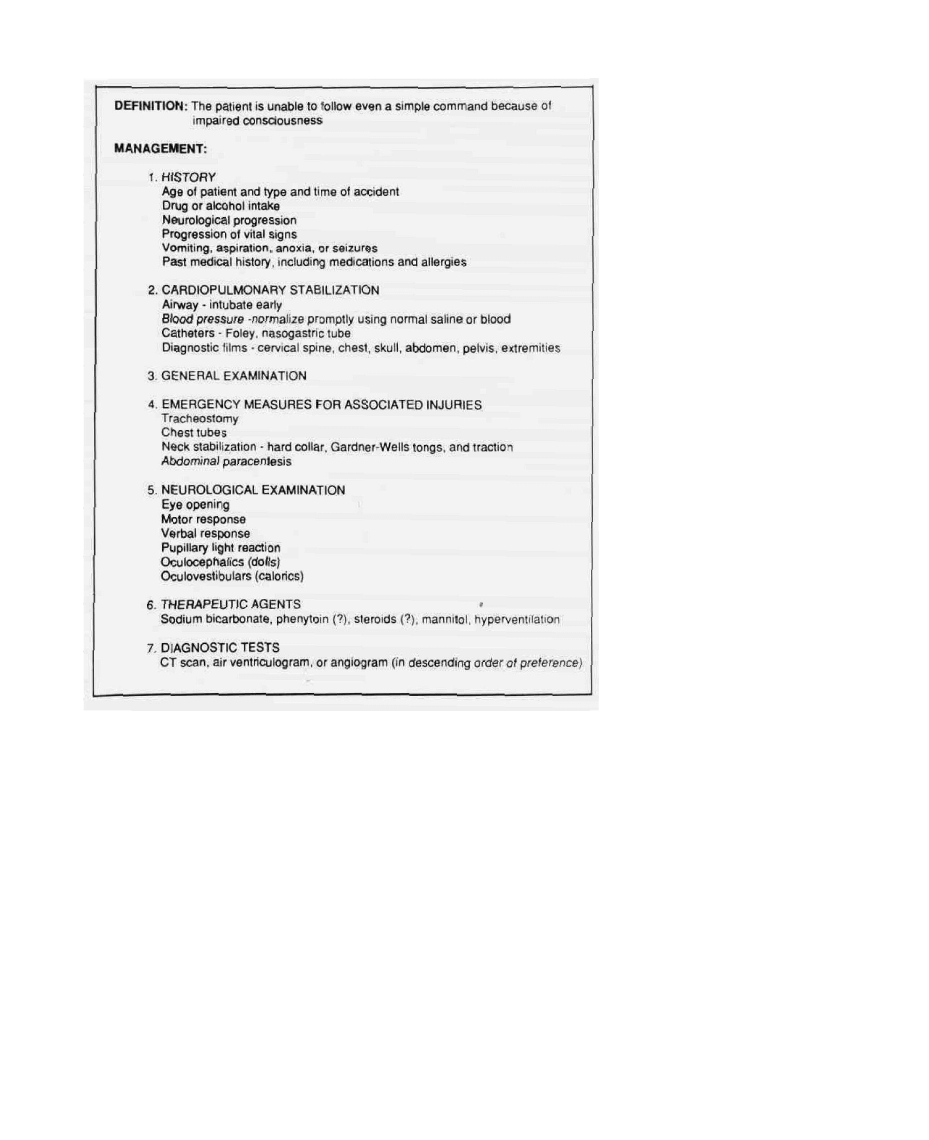
Severe Head Injury
This group consists of patients who are unable to fol-
low simple commands even after cardiopulmonary sta-
bilization. Although this definition is inclusive of a fairly
wide spectrum of brain injury, it identifies a group of
patients who are at maximal risk of suffering significant
FIG. 3. Management of moderate head injury.
242
CHAPTER 12
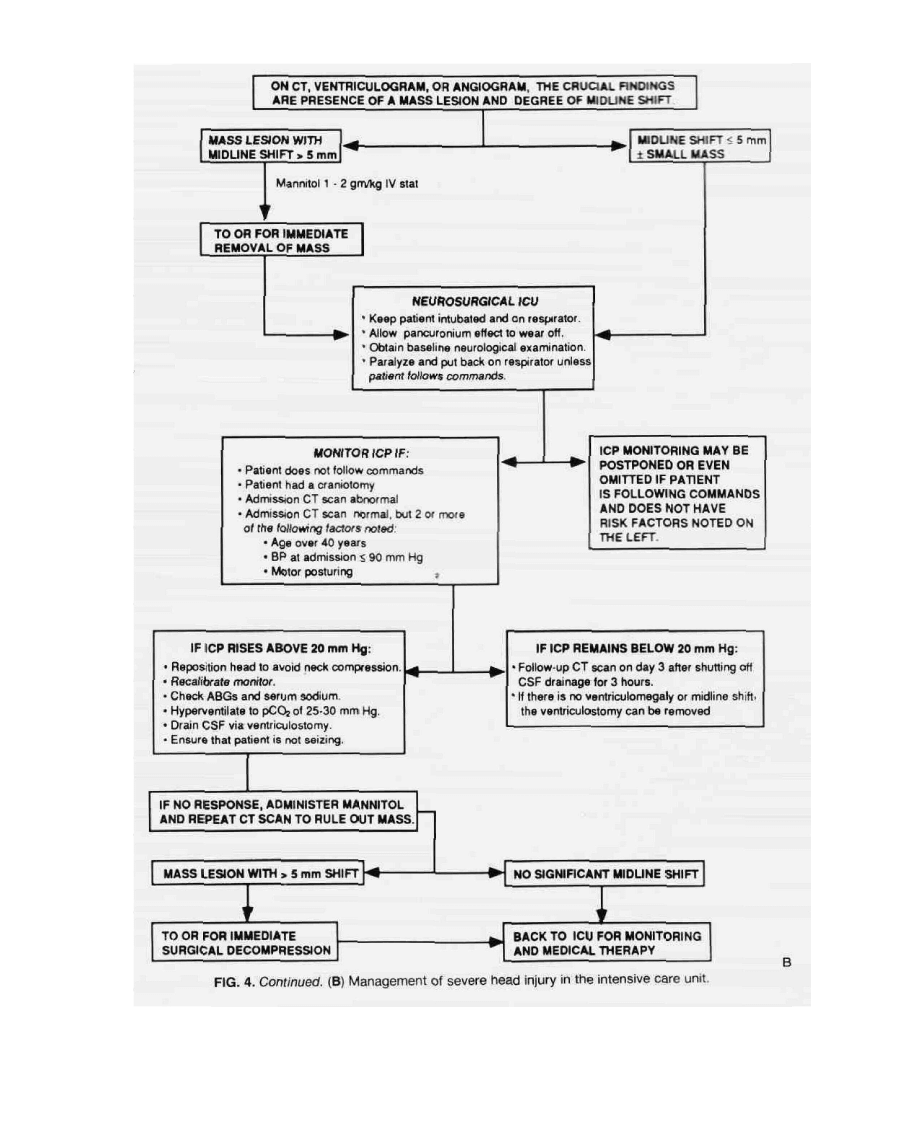
FIG. 4. (A) Management of severe head
injury in the emergency room. FIG. 4.
continues on p. 243 .
morbidity and mortality. We believe that in such pa-
tients a "wait and see" approach can be disastrous and
that prompt diagnosis and treatment is of the utmost
importance (17,28,29) (Fig. 4). The management of
these patients is described in five stages: (1) cardiopulmo-
nary stabilization, (2) general examination, (3) neurologi-
cal examination, (4) diagnostic procedures, and (5) indi-
cations for surgery.
90 mm Hg) is one of the three factors in severely head
injured patients with a normal CT scan (the other two
being age > 40 years and motor posturing) that, when
noted at admission, is associated with subsequent intra-
cranial pressure (ICP) elevation. High ICPs are in turn
associated with poorer outcomes (30). It is imperative,
therefore, that cardiopulmonary stabilization be
achieved rapidly.
Cardiopulmonary Stabilization
Brain injury is often adversely affected by secondary
insults. Miller and associates reported that, of 100 consec-
utive patients with severe brain injury evaluated on ar-
rival in the emergency room, 30 percent were hypoxemic
(Po
2
< 65 mm Hg), 13 percent were hypotensive (sys-
tolic BP < 95 mm Hg), and 12 percent were anemic
(hematocrit < 30%) (10). It has subsequently been dem-
onstrated that hypotension at admission (systolic BP <
Airway
A frequent concomitant of concussion is transient re-
spiratory arrest. Prolonged apnea may often be the cause
of "immediate" death at the scene of an accident. If arti-
ficial respiration can be immediately instituted, a good
outcome can result (31). Apnea, atelectasis, aspiration,
and acute respiratory distress syndrome (ARDS) are fre-
quently associated with severe head injury, and by far the
single most important aspect of the immediate manage-
HEAD INJURY / 243
244 / CHAPTER 12
ment of these patients is the establishment of a reliable
airway (32). All severely head-injured patients should be
intubated immediately. Care should be taken to ensure
proper endotracheal, rather than esophageal, placement
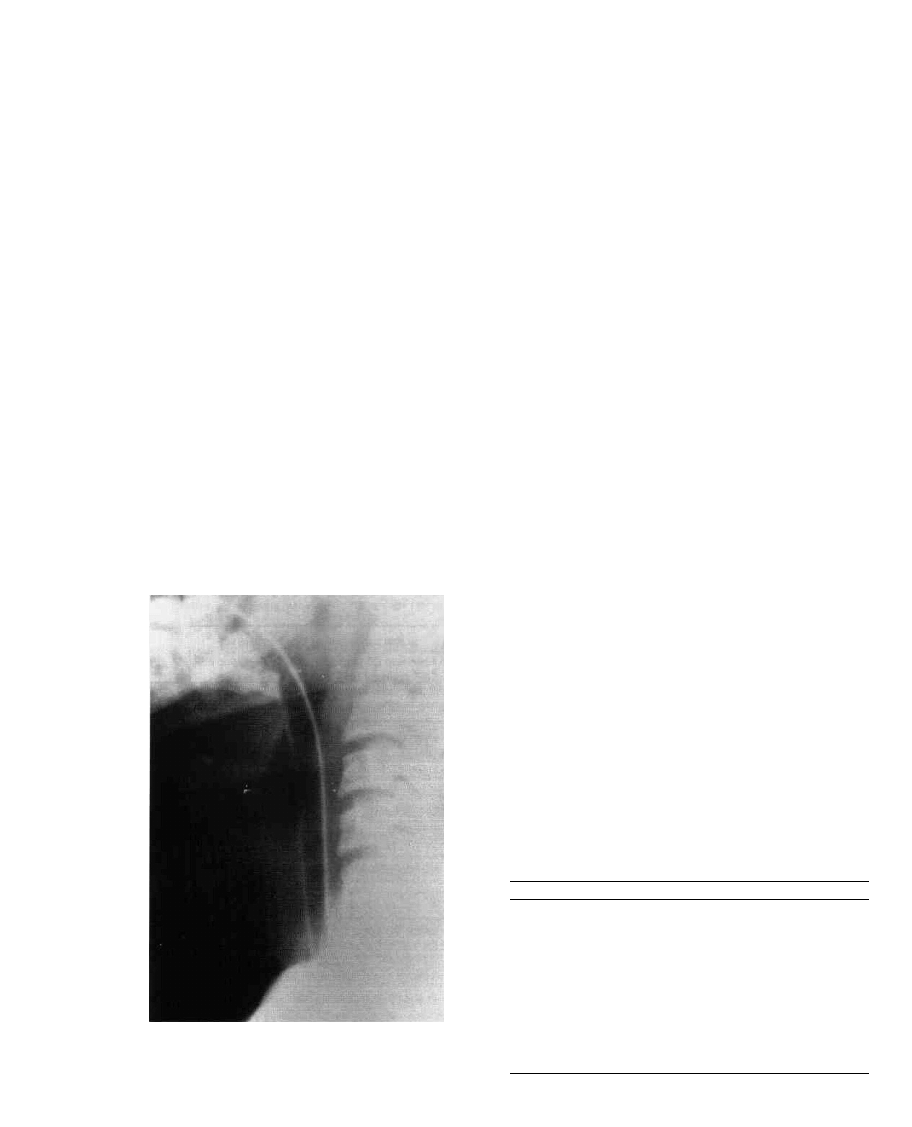
of the tube (Fig. 5). Infrequently, it is necessary to per-
form an emergency tracheostomy, especially in patients
with severe maxillofacial injuries in whom intubation
may be precluded because of severe soft tissue swelling
and distortion of the anatomy (33).
In the process of establishing an airway, the mouth
and nasal passages must be cleared of all foreign bodies,
secretions, blood, and vomitus. Once the endotracheal
tube is in place, the cuff should be blown up to prevent or
reduce aspiration, and a thorough suctioning of the tra-
cheal passages should be performed. One hundred per-
cent oxygen is then used for ventilation until blood gases
can be checked and appropriate adjustments of the FIO2
made. There is little danger of oxygen toxicity if 100
percent oxygen is used for less than 48 to 72 hours (34).
Blood Pressure
Hypotension and hypoxia are the principal enemies of
the head-injured patient. It has recently been shown that
the presence of hypotension (systolic BP < 90 mm Hg) in
severely head-injured patients increases the mortality
jte from 27 percent to 50 percent (35). Furthermore, it
waslbund that 35 percent of patients arriving at major
trauma centers are hypotensive. While the airway is be-
ing established, another group of ER personnel should
be checking the patient's pulse and blood pressure and
taking steps to obtain venous access. A minimum of two
intravenous lines (using 14- or 16-gauge Jelcos) should
be promptly placed. We generally use a percutaneous
infraclavicular subclavian or a jugular venous catheter
(36,37), although occasionally a saphenous or brachial
vein cutdown may be necessary to provide reliable ve-
nous access. At this point, blood may be drawn for a
CBC, SMA 20, coagulation screen, serum alcohol level,
sample to the blood bank, and arterial blood gases.
If the patient is hypotensive, it is of vital importance to
restore normal blood pressure as soon as possible. Hypo-
tension is usually not due to the brain injury per se, ex-
cept in the terminal stages when medullary failure super-
venes. Far more commonly, hypotension is a marker of
severe blood loss, which may be "overt," "occult," or
possibly both (Table 3).
In the hypotensive traumatized patient, one must con-
sider associated spinal cord injury (with quadriplegia or
paraplegia) as well as cardiac contusion or tamponade
and tension pneumothorax as possible causes. While ef-
forts are in progress to determine the cause of the hypo-
tension, volume replacement should be initiated using
normal saline and plasmanate. Blood transfusions must
be started as soon as possible when the blood pressure
does not respond promptly to fluid replacement or when
the hemoglobin level is found to be less than 10.0 gm%
(HCT 30%). Group O Rh negative blood may be used
pending cross-matched blood availability. The impor-
tance of routine abdominal paracentesis in the hypoten-
sive comatose patient has been demonstrated (38).
It must be emphasized that a patient's neurological
examination is meaningless as long as he or she is hypo-
tensive. Time after time we have seen patients who are
unresponsive to any form of stimulation while hypoten-
sive revert to a near-normal neurological examination
fairly soon after normal blood pressure is restored.
TABLE 3. Common sites of blood loss in the
multiple trauma patient
1.
2.
3.
4.
Overt
Scalp lacerations
Maxillofacial injuries
Compound fractures
Other soft-tissue injuries
1 .
2.
3.
4.
5.
6.
Occult
Intraperitoneal or
retroperitoneal
Hemothorax
Pelvic hematoma
Bleeding into extremities
at site of long-bone
fractures
Subgaleal or extradural
hematoma in an infant
Traumatic rupture of
the aorta
FIG. 5. Esophageal intubation. Lateral cervical film of an en-
dotracheal tube that was erroneously placed in the esopha-
gus. Note the tracheal air shadow anterior to the tube.
HEAD INJURY / 245
Catheters
A Foley catheter (16-18 French for average adults)
should be carefully inserted and urine sent for urinalysis
and toxic screen (when appropriate). Gross hematuria
suggests renal injury and is an indication for an emer-
gency IVP. Mild hematuria may be secondary to trau-
matic catheterization, to renal contusion, or, rarely, to a
dissecting aortic aneurysm. Despite, and perhaps be-
cause of, the general air of agitation associated with the
arrival of a trauma victim in the emergency room, spe-
cial attention must be paid to maintaining reasonably
accurate records of fluid intake and output, especially in
children and in the elderly. In addition to ensuring fluid
balance, such records help assess blood loss and monitor
renal perfusion.
A nasogastric tube, preferably a Salem sump (double-
lumen plastic catheter), should be inserted and con-
nected to a wall suction. Potential complications of this
procedure, such as intracranial passage of the tube sec-
ondary to a basal skull fracture, must be kept in mind
(39,40). In patients with anterior basal skull fractures it is
probably wise to pass the tube under direct vision with a
laryngoscope or to pass it per orum.
»
Diagnostic X-Rays
As soon as the preliminary steps towards cardiopulmo-
nary stabilization have been taken, the following x-rays
should be obtained.
Cervical Spine (Cross-Table Lateral and Anteroposte-
rior). These are the first films to be taken in the severely
traumatized patient and must be read by a radiologist or
neurosurgeon before the patient's neck can be moved.
Features to look for in this study are ( 1 ) loss of alignment
of the vertebral bodies, (2) bony fractures or compres-
sion, (3) loss of alignment of the facet joints, and (4)
prevertebral soft-tissue swelling (more than 5 m m oppo-
site the C3 vertebral body is significant). Every effort
must be made to visualize the lower cervical levels (C6 to
C7, C7 to Tl) because these are often obscured by the
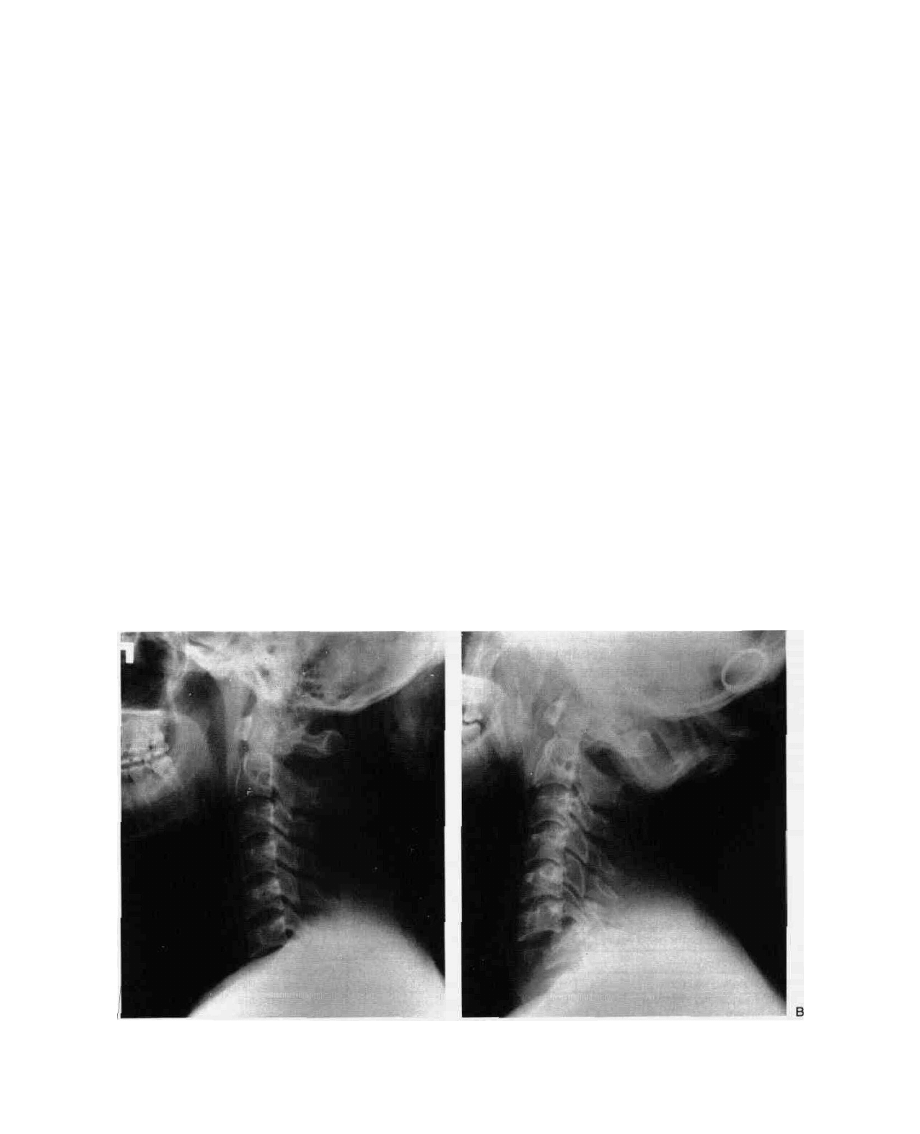
shoulders, especially in heavy-set patients. Fracture sub-
luxations at these levels may be overlooked if the films
are not repeated with caudad traction on both arms and
greater x-ray penetration (Fig. 6). If these maneuvers also
fail, a "swimmer's view" can be obtained. If these films
show any of the abnormalities in the preceding list, the
neck must remain immobilized in a hard collar (Philadel-
phia) pending further studies (high-resolution CT scan
or polytomogram).
Chest. This important film is useful in ruling out (1)
endotracheal tube malposition, (2) pneumothorax, (3)
hemothorax, (4) lung contusion, (5) hemopericardium,
(6) rib fractures. (7) thoracic spine fractures, and (8)
other thoracic pathology that may have a bearing on pa-
tient management.
Skull (Anteroposterior and Lateral). These are useful,
as discussed earlier, although their value has been some-
what overshadowed by CT scanning. They help in iden-
tifying maxillofacial injuries, depressed skull fractures.
FIG. 6. Missed C7 fracture-subluxation. The importance of pulling the shoulders down or obtaining a
swimmer's view is demonstrated in this example of an unstable cervical injury that would have been
ilssed (A) had a repeat film not been obtained (B).
246 / CHAPTER 12
and penetrating injuries. The presence of intracranial air
(pneumocephalus) or of an air-fluid level in one of the
sinuses can alert the clinician to a basal skull fracture
that might otherwise have gone undetected.
Abdominal. A single anteroposterior abdominal film
(KUB) is usually taken in trauma patients. This can help
rule out (in a gross way) large retroperitoneal hemato-
mas, lumbosacral spine fractures, distended viscera, and
possibly subdiaphragmatic air.
Pelvic. Anteroposterior and lateral pelvic films are
usually obtained, looking for pelvic injuries that may be
the site of significant blood loss.
Extremities. These may be studied whenever indi-
cated to rule out fractures or subluxations.
General Examination
During the process of cardiopulmonary stabilization,
the clinician conducts a rapid general examination look-
ing for other injuries. In one series of severely head-in-
jured patients, more than 50 percent had additional ma-
jor systemic injuries requiring care by other specialists
(10) (Table 4). Particular attention should be paid to
1. Head and neck injuries: lacerations, bleeding sites,
otorrhea, rhinorrhea, raccoon eyes (periorbital ecchy-
mosis), or Battle's sign (retroauricular ecchymosis).
2. Thoracic injuries: rib fractures, pneumothorax or he-
mothorax, cardiac tamponade (with soft heart
sounds, jugular venous distension, and hypotension),
aspiration, or ARDS.
3. Abdominal injuries: especially liver, spleen, or kidney
lacerations. Hemorrhage usually results in abdominal
tenderness, guarding, or distension. However, these
signs may not manifest early and may be obscured in
the comatose patient. The presence of bowel sounds
is usually a reassuring sign.
4. Pelvic injuries: Injuries in noncomatose patients may
be ascertained clinically. Radiological confirmation
is usually necessary. Rectal examination may be use-
ful. Pelvic injuries are often associated with signifi-
cant occult blood loss.
5. Spinal injuries: Head and spinal trauma may coexist,
and this combination must always be searched for
even though it is infrequent, occurring in 2 to 5 per-
cent of severely head-injured patients (41,42). In
TABLE 4. Systemic injuries in WO patients with
severe head injury
3
Type of injury
Long-bone or pelvic fracture
Maxillary or mandibular fracture
Major chest injury
Abdominal viscera injury
Spinal injury
Incidence (%)
32
22
23
7
2
a
Adapted from reference 10, with permission.
these patients, the cervical spine is most frequently
involved (43,44).
6. Injuries involving extremities: These may consist of
bony or soft-tissue (muscle, nerve, blood vessel) dam-
age. The agitated patient should have fractures
splinted promptly to prevent damage to contiguous
nerves and vessels. Definitive treatment of most inju-
ries involving the extremities can be postponed until
after treatment of more life-threatening problems.
Neurological Examination
As soon as the patient's cardiopulmonary status has
been stabilized, a rapid and directed neurological exami-
nation is performed (Table 5). Although various factors
can prevent an accurate evaluation of the patient's neuro-
logical state at this point (e.g., hypotension, hypoxia, or
intoxication), valuable data can nevertheless be obtained
(45). Between the fully alert and the deeply comatose
patient lies a continuum of altered consciousness that is
difficult to quantify objectively. As noted earlier, the
Glasgow Coma Scale is widely used for this purpose.
If a patient demonstrates variable responses to stimula-
tion, or if the response on each side is different, the best
response appears to serve as a more accurate prognostic
indicator than does the worst response (Table 6). To fol-
low trends in an individual patient's progress, however,
it is better to report both the best and the worst re-
sponses. In other words, the right-sided and left-sided
motor responses should be recorded separately (46). As
the pain stimulus applied by different examiners is often
quite variable, deep nail-bed pressure should be used as
the standard stimulus.
The physician should not limit the examination to the
parameters of unconsciousness that are used in the GCS,
however, (i.e., eye opening, motor response, and verbal
response) (Table 7). Of equal importance in the initial
assessment of patients with impaired consciousness are
the patient's age, vital signs, pupillary response, and eye
movements (45). The GCS provides a simple grading of
the arousal and functional capacity of the cerebral cor-
tex, and the pupillary responses and eye movements
serve as measures of brainstem function. Advanced age,
hypotension, and hypoxia all adversely affect outcome
(30). Indeed, there is considerable interplay among all
these factors in determining the ultimate prognosis in
the severely head-injured patient.
TABLE 5. Initial neurological examination in head injury
1 . Glasgow Coma Scale
2. Pupillary response to light
3. Eye movements
a. Oculocephalic (dolls)
b. Oculovestibular (calorics)
4. Motor power
5. Gross sensory examination
HEAD INJURY / 247
TABLE 6. Comparison of outcome with different motor responses
3
Motor response
Not posturing or flaccid
Uni- or bilaterally decorticate
Uni- or bilaterally decerebrate
Bilaterally flaccid
Total
# Cases
83
20
19
11
133
G/MD
C
74
60
21
27
60
Outcome (%)
SD/V
C
7
5
16
9
8
Dead
19
35
63
64
32
a
From reference 45, with permission.
b
G = good outcome; MD = moderately disabled
0
3D = severely disabled; V = vegetative
Pupils
Careful notation of pupil size and response to light is
of utmost importance during the initial examination. A
well-known early sign of temporal lobe herniation is
mild dilation of the pupil and a sluggish pupillary light
response. Either compression or distortion of the oculo-
motor nerve during tentorial-uncal herniation impairs
the function of the parasympathetic axons that transmit
efferent signals for pupillary constriction (47), resulting
in mild pupillary dilation. However, bilateral miotic pu-
pils (1 to 3 mm) occur in the early stages of central ce-
phalic herniation (48). This is due to bilateral compro-
mise of the pupillomotor sympathetic pathways
originating in the hypothalamus, permitting a predomi-
nance of parasympathetic tone and pupillary constric-
tion. In either instance, continued herniation causes in-
creasing dilation of the pupil and paralysis of its light
response. With full mydriasis (8 to 9 mm pupil), ptosis
and paresis of the medial rectus and other ocular muscles
innervated by the oculomotor nerve appear. A bright
light is always necessary to determine pupillary light re-
sponses. A magnifying lens such as the plus-20-diopter
lens on a standard ophthalmoscope is helpful in distin-
guishing between a weak pupillary light reaction and ab-
sence of a reaction, especially if the pupil is small.
TABLE 7. Outcomes associated with different clinical features noted soon after admission in severe head injury*
Outcome (%)
" From reference 45, with permission.
" G = good recovery; MD = moderately disabled
c
SD = severely disabled; V = vegetative
"p<0.02
8
GCS = Glasgow Coma Scale
' p < 0.0002
1.
2.
3.
4.
5.
6.
Clinical features
Age"
0-20
21-40
41-60
61 +
GCS" admission score'
3-5
6-8
9-11
1 2 - 1 4
Pupillary reaction'
Normal
Bilaterally impaired
Eye movements'
Normal
Unilaterally or bilaterally impaired
Surgical decompression'
None
Once
Two or three times
Motor posturing"
None (includes flaccidity)
Unilateral or bilateral
# Cases
46
50
28
9
39
74
17
3
87
46
74
57
74
47
1 2
94
39
G/MD"
72
66
43
22
23
74
76
100
76
30
76
39
76
47
17
68
41
SD/V
C
11
6
1 1
0
15
6
6
0
8
9
7
10
7
11
8
7
10
Dead
17
28
46
78
62
20
18
0
16
61
17
51
17
42
75
25
49

CHAPTER 1!
Recognition of additional pupillary disorders that can
occur in an unconscious patient is useful in the examina-
tion of a patient with head trauma. Hippus is an unex-
plained phenomenon consisting of spontaneous dilation
and contraction of the pupil, and it is often observed in
patients with Cheyne-Stokes respirations. Rather than
indicating disordered function, however, it suggests
functional integrity of sympathetic-parasympathetic pu-
pillary pathways. Disruption of the afferent arc of the
pupillary light reflex within the optic nerve is detected by
employing the swinging flashlight test (49). As the flash-
light is swung from the normal to the injured eye, injury
to the optic nerve is indicated by a paradoxical response
of the pupil: dilation rather than constriction. Appar-
ently, light signals transmitted to the Edinger-Westphal
nucleus in the midbrain through the injured optic nerve
are insufficient to maintain the constriction brought
about by illumination of the normal eye. The paradoxi-
cal pupillary dilation observed as the light is moved from
the normal to the abnormal eye is termed an afferent
pupillary defect, or Marcus-Gunn pupil, and in the ab-
sence of opacification of the ocular media it is unequivo-
cal evidence of optic nerve injury.
Bilateral small pupils suggest that the patient has used
certain drugs, particularly opiates, or has one of several
metabolic encephalopathies or a destructive lesion of the
pons (50). In these conditions pupillary light responses
usually can be seen if examined with a magnifying lens.
The miosis that occurs with a pontine lesion apparently
results from structural or physiological inactivation of
sympathetic pathways descending from the hypothala-
mus through the reticular activating system to the spinal
cord. Unilateral Horner 's pupil is seen occasionally with
brainstem lesions, but in the trauma patient attention
should be given to the possibility of a disrupted efferent
sympathetic pathway at the apex of the lung, base of the
neck, or ipsilateral carotid sheath. Midposition pupils
with variable light responses are observed in all stages of
coma. Traumatic oculomotor nerve injury is the diagno-
sis in patients with a history of a dilated pupil from the
onset of injury, with an improving level of conscious-
ness, and with appropriate ocular muscle weakness (51).
A mydriatic pupil (6 mm or more) occurs occasionally
with direct trauma to the globe of the eye. This traumatic
mydriasis is usually unilateral and is not accompanied
by ocular muscle paresis. Rarely recognized is the corec-
topic pupil associated with midbrain disorders. In this
sign, the pupillary aperture appears to migrate within the
iris stroma as various sectors of the iris musculature con-
tract and relax asynchronously (52).
Finally, bilaterally dilated and fixed pupils in patients
with head injury may be the result of inadequate cerebral
vascular perfusion. This situation can be caused by hy-
potension secondary to blood loss or by elevation of in-
tracranial pressure to a degree that impairs cerebral
blood flow. Return of the pupillary response may occur
promptly after the restoration of blood flow if the period
of inadequate perfusion has not been too long.
Eye Movements
Ocular movements are an important index of the
functional activity that is present within the brainstem
reticular formation. If the patient is sufficiently alert to
follow simple commands, a full range of eye movements
is easily obtained, and the integrity of the entire ocular
motor system within the brainstem can be affirmed. In
states of depressed consciousness, voluntary eye move-
ment is lost, and there may be dysfunction of the neural
structures activating eye movements. In these instances,
oculocephalic or oculovestibular responses are used to
determine the presence or absence of an eye-movement
disorder. To employ these tests, an understanding of the
anatomical connections involved in the normal response
is necessary.
Anatomy. Clinicians have long realized that a conju-
gate gaze center controlling ipsilateral horizontal fast eye
movements (saccades) and vestibular responses lies
within the lower paramedian pontine reticular formation
(53). This region includes a pulse generator for fast eye
movements and a neural integrator that determines the
ultimate resting position of the eye. Recent studies in
cats show that the caudal portion of the horizontal gaze
center extends into the nucleus prepositus hypoglossi in
the rostral medulla and that it significantly participates
in saccadic vestibular and voluntary slow eye move-
ments (54). Thus, clinical and animal investigations indi-
cate that the final common pathway for all ipsilateral
conjugate horizontal eye movements is located within
the tegmentum of the paramedian pontomedullary junc-
tion. From here, signals for horizontal eye movements
are transmitted to the nearby ipsilateral abducens nu-
cleus and cross the midline in the para-abducens region
to ascend in the contralateral medial longitudinal fascicu-
lus to the medial rectus neurons in the oculomotor nu-
cleus (55).
Oculocephalic response. In an unconscious patient
with trauma to the head, loss of horizontal eye move-
ment indicates the need for urgent diagnostic study. If a
neck fracture has been excluded, function of the pontine
gaze center is quickly ascertained by the oculocephalic
maneuver. The head is raised 30 degrees from the supine
position and briskly rotated to and fro in the horizontal
plane. In the normal doll's-eyes response, both eyes tend
to maintain their position in space by moving opposite
to the rotation of the head and horizontally toward their
respective lateral and medial positions in the orbit. As
this maneuver is performed, the eyelids may be man-
ually retracted to better observe movements of the globe.
Afferent impulses from cervical nerve roots and the
semicircular canals contribute to the normal compensa-

HEAD INJURY / 249
tory reflexes that shift the eyes in the direction opposite
to rotation of the head. Impairment or absence of the
oculocephalic response may be due to malpositioning or
inadequate head rotation. Some patients whose oculoce-
phalic responses are impaired or absent will have normal
caloric responses. Therefore, all patients with impaired
oculocephalic responses, in addition to those in whom
neck fracture has not been ruled out and who therefore
cannot be tested for this response, should have caloric
stimulation of oculovestibular pathways.
Oculovestibular response. This stimulation can be ac-
complished with ice water and only a small expenditure
of time. Obstructions within the external auditory canal
of blood or cerumen need to be removed. Limitation of
ocular muscle movement occurs in patients with orbital
edema. Intraorbital swelling is usually obvious to the ex-
aminer but should not discourage use of oculocephalic
or caloric testing. Much information can still be gained.
Movement of endolymph within the horizontal semicir-
cular canal acts primarily upon conjugate movement of
the medial and lateral rectus muscles (56). To produce
maximal shift of this fluid during caloric stimulation, the
horizontal canal is positioned in the vertical plane by
lifting the patient's head 30 degrees from the supine posi-
tion. The temperature gradient between the irrigating
fluid and the endolymph produces movement of the lat-
ter within the semicircular canal. Normally, this occurs
within 20 to 60 seconds and lasts several minutes. Warm
water irrigation of the external canal causes endolym-
phatic fluid to rise, which causes contralateral tonic de-
viation of the eyes. Irrigation with cold water causes the
endolymph to fall, and this causes ipsilateral tonic gaze
deviation.
Although direct connections between vestibular and
ocular neurons are known, tonic eye deviation following
caloric stimulation is likely to be the result of complex
interactions within the eye-movement control systems
of the pontomedullary reticular system. In alert patients,
cold caloric stimulation causes fast-phase nystagmus in
the direction opposite the tonic eye deviation. The mne-
monic "cows"—cold opposite, warm same—refers to
this condition. However, in comatose patients, func-
tional suppression of the reticular activating system is
reflected by the absence of nystagmus in response to calo-
ric stimulation, so only the tonic eye deviation is seen
(cold same). Use of 20 ml of ice water suffices, but if no
response occurs within one minute, it is best to repeat the
test with a larger volume. If the second irrigation does
not elicit eye movement, simultaneous oculocephalic
maneuvers can be used to enhance the stimulus. To elim-
inate semicircular canal or vestibular nerve injury as the
cause of absence of cold caloric responses, normal warm
water caloric responses of the opposite ear may be ob-
tained.
Full oculocephalic responses in the unconscious pa-
tient indicate that the process producing the coma spares
the paramedian pontine reticular formation, the medial
longitudinal fasciculus, and the oculomotor and abdu-
cens nuclei and their nerve roots. Moreover, the suppres-
sion of the reticular activating system responsible for the
loss of consciousness is assumed to be operant rostral to
these pontine and midbrain structures. An intermediate
response, i.e., absence of oculocephalic responses but in-
tact caloric responses, has been reported to occur with
supratentorial lesions (57). Absence of both oculocepha-
lic and caloric responses indicates a severe pathological
process extending to the lower pons.
While oculocephalic and caloric testing is being per-
formed, infranuclear, internuclear, and supranuclear oc-
ular motility disorders are recognizable. A destructive le-
sion of either a frontal or a pontine gaze center results in
tonic overact ion of the opposite frontal-pontine axis for
horizontal eye movement. Tonic deviation of the eyes
occurs from the action of the spared frontal-pontine sys-
tem. This overaction results in ipsilateral deviation of
the eyes with frontal lobe lesions and contralateral gaze
deviation with pontine lesions. In deep coma, gaze de-
viation owing to the overbalance is not necessarily pres-
ent. To distinguish between a possible frontal or pontine
lesion in patients with or without gaze deviations, oculo-
cephalic and caloric testing is needed. In gaze deviations
caused by frontal lobe lesions, oculocephalic and caloric
reflexes remain intact because vestibular input into the
paramedian pontine reticular formation is preserved.
Pontine lesions interrupt oculocephalic and oculovesti-
bular-paramedian pontine reticular formation interac-
tion so that rotation of the head toward the deviated eye
or cold water irrigation of the ear contralateral to the
gaze deviation does not overcome the gaze deviation.
Incomplete or paretic conjugate horizontal gaze follow-
ing appropriate caloric stimulation suggests a partially
damaged pontine gaze center. Dysconjugate oculoce-
phalic and oculovestibular responses are due to either a
third or a sixth cranial nerve palsy or to internuclear
ophthalmoplegia if only one horizontal muscle is pare-
tic. If both horizontal muscles for conjugate gaze are par-
etic but one more than the other, a perverted form of a
pontine gaze palsy is present.
Skew deviation is divergence of the eyes in the vertical
plane and is a sign of a lesion within the brain stem. An
explanation for the tonic and vertical deviation of one or
both eyes is not known. In skew deviations, neuroana-
tomical localization within the brainstem is not ordi-
narily possible by notation either of the downward, or
hypometric, eye or of the upward, or hypermetric, eye.
Generally, third and sixth nerve palsies are not diffi-
cult to recognize in patients with head injury. Fourth
nerve palsies cannot ordinarily be identified in coma be-
cause of the select action of the superior oblique muscle.
In the alert and recovering patient, however, superior
oblique paresis causes troublesome double vision, espe-
cially with downward and inward gaze. Head tilt oppo-

250 / CHAPTER 12
site the side of the paretic muscle lessens the double vi-
sion, while ipsilateral tilt of the head increases diplopia.
Internuclear ophthalmoplegia is suggested by select ad-
duction paresis without additional involvement of the
pupil, lid, or vertical muscles innervated by the third
nerve. This ophthalmoplegia results from disruption of
the ipsilateral medial longitudinal fasciculus that con-
nects the oculomotor subnucleus for medial rectus neu-
rons to the contralateral horizontal gaze center. Either
bilateral or unilateral internuclear ophthalmoplegia may
be seen, depending upon the extent of the brainstem
trauma.
Little is known about the incidence of vertical gaze
palsies in coma states. Downward eye deviation is rare in
head injury but may be associated with posterior thala-
mic hemorrhage. Failure of upward gaze is, however,
occasionally seen in patients with bilateral subdural he-
matomas or hydrocephalus, and it is thought to repre-
sent compression of the tectal plate. With unilateral cold
caloric testing, downward deviation of the eyes has been
reported in coma caused by drug intoxication (57). Ver-
tical gaze is tested by manually rotating the head in the
vertical plane. This maneuver normally results in com-
pensatory up-and-down gaze. Simultaneous irrigation of
both ears activates the semicircular canals to cause verti-
cal response; bilateral cold water tests produce tonic up-
ward movement of the eyes, and bilateral warm water
tests produce tonic downward gaze.
Motor Function
The basic examination is completed by a gross test of
motor strength because severely head-injured patients
are not sufficiently responsive for such a determination
to be reliably made. Each extremity is examined and
graded on the internationally used scale as follows:
Normal power 5
Moderate weakness 4
Severe weakness (antigravity) 3
Severe weakness (not antigravity) 2
Trace movement 1
No movement 0
Diagnostic Procedures
As soon as a patient's cardiorespiratory condition has
been stabilized and a preliminary neurological examina-
tion completed, it behooves the physician to rule out the
presence of an intracranial mass lesion. The patient is by
this time intubated and should be paralyzed with pan-
curonium (Pavulon) or a similar agent and put on me-
chanical ventilation. This maneuver prevents the patient
from straining and moving around, thus avoiding intra-
cranial pressure surges and greatly enhancing the quality
of the diagnostic studies. Needless to say, CT scanning
has rendered all other diagnostic tests virtually obsolete.
However, other tests have to be used in certain instances
either to substitute for CT scanning or, as in the case of
angiography, to obtain certain supplemental data.
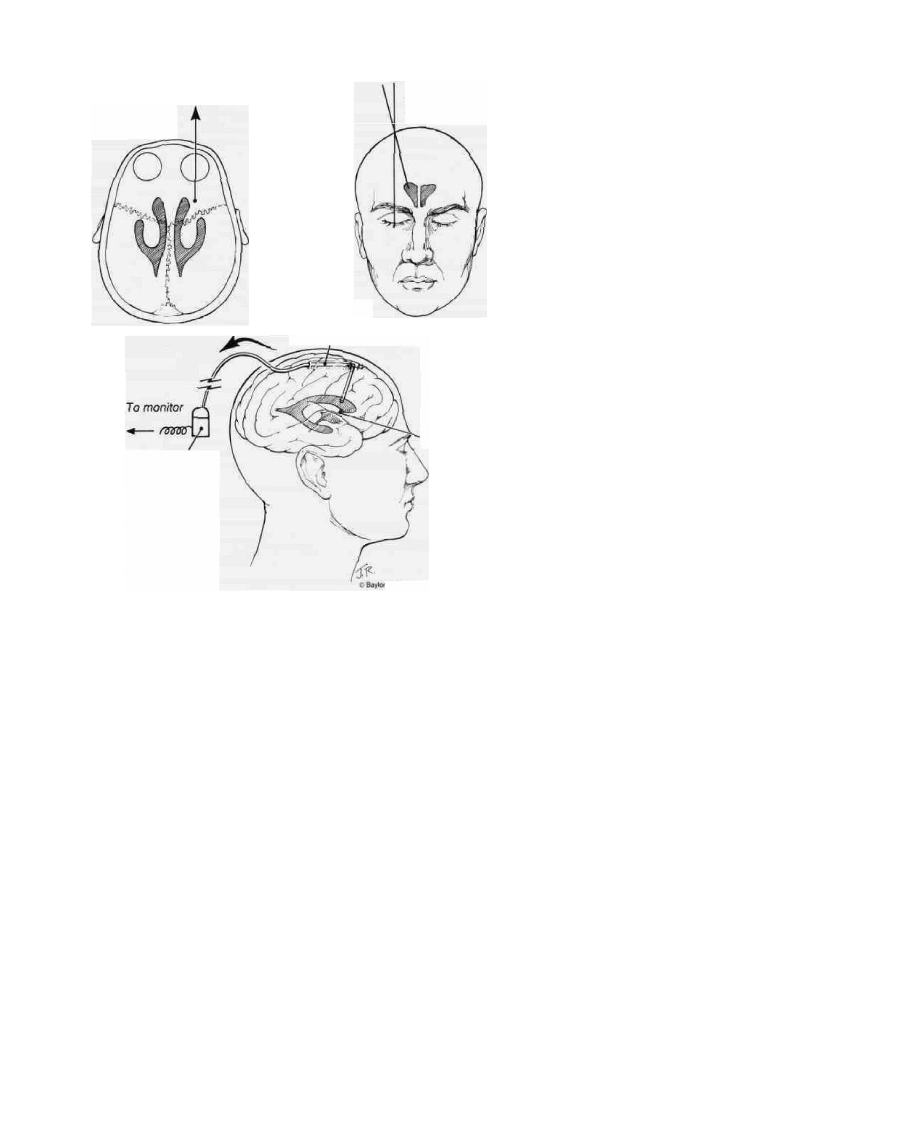
Ventriculography
Prior to the advent of CT scanning, air ventriculogra-
phy and angiography were the most important emer-
gency radiological tests for evaluating comatose head-in-
jured patients. The former was favored because of the
rapidity with which it could be obtained, even though
the latter could provide more information. Ventriculog-
raphy provides two crucial pieces of information: the
degree of supratentorial brain shift and the intracranial
pressure. If the procedure is performed in a methodical
and standardized fashion, the ventricle can almost al-
ways be cannulated to provide a satisfactory ICP mea-
surement and air study, even when the patient has a ma-
jor ventricular shift or slit-like ventricles secondary to
compression.
Technique. If there are no focal signs that favor a uni-
lateral mass lesion, the right side should be chosen. If,
however, there is reason to believe there is a mass on a
given side, the opposite side should be used because it is
easier to cannulate the less compressed ventricle. The
scalp is shaved widely in the region of the coronal suture.
After prepping the area with betadine solution and drap-
ing it with sterile towels, a 1-cm incision is made in the
scalp just anterior to the coronal suture in the midpupil-
lary line (Fig. 7). Using a 9/64 drill bit on a twist-drill set,
a small hole is made through the skull at this point. The
drill is directed towards the nasion, and in the sagittal
plane toward the opposite ear. The length of the drill bit
is adjusted to about 2 to 2.5 cm to avoid plunging into
brain material. As soon as the drill has penetrated the
skull a "give" is felt and the drill withdrawn. The dura is
best entered with a hand-held smaller drill bit using a
twisting motion. A manometer is filled with sterile saline
to a level of around 300 mm of water and connected to a
flexible tube with a stopcock. A No. 16 brain cannula or
a ventriculostomy tube is then passed through the hole
directed towards the lateral ventricle. The axes used are
as stated—toward the nasion and the opposite ear. If the
ventricle is not entered with this pass, the axis is biased
toward the ipsilateral pupil and then toward the contra-
lateral pupil in the next two passes. The ventricle should
be entered around 7 to 8 cm; deeper passes are inadvis-
able. Once the cannula has been passed, the stylet is par-
tially withdrawn to confirm entry into the ventricle. If
the cannula is in the ventricle, cerebrospinal fluid will be
seen flowing out as the stylet is withdrawn. Care should
be taken to avoid losing more than a drop or two of CSF
while withdrawing the stylet and connecting on the ma-
nometer tube, so as to obtain the most accurate ICP
HEAD INJURY
A. Entry Site
B. APView
C. Ventriculostomy
Tunnel under scalp
Foramen of Monro
Pressure transducer
College of Medicine 1990
readings. If all three passes on one side fail to enter the
ventricle, the procedure is repeated on the other side. If
three passes on the other side also fail, the procedure is
abandoned.
Once the manometer is connected onto the cannula,
the stopcock is opened and the ICP is measured with the
patient lying flat on his or her back. The foramen of
Monro is used as the point of reference. It should be
remembered that arterial hypotension may be reflected
in low ICP readings and that hypercarbia and hypoxia
tend to raise ICP. After measuring the pressure, approxi-
mately 7 cc of air is carefully exchanged for CSF, the
head is tilted from side to side, and a brow-up anteropos-
terior Townes projection skull x-ray is obtained after re-
moving the cannula and closing the scalp incision with a
single suture.
Normal ICP in a relaxed or paralyzed patient who is
neither hypotensive nor hypercarbic/hypoxic is 10 mm
Hg (136 mm H
2
O) or less. Although pressures in the
range of 10 to 20 mm Hg (136 to 272 mm H
2
O) may
occur with moderate disturbances of intracranial vol-
umes, pressures greater than these warn of a major intra-
cranial hematoma, serious diffuse brain injury, or both
(46). A major change in intracranial pressure-volume dy-
namics is required to raise intracranial pressures to these
levels.
FIG. 7. Anatomical landmarks for a ventriculo-
gram. For the preferred frontal approach, a twist-
drill hole is made in the midpupillary line just ante-
rior to the coronal suture (A). The drill is directed
towards the nasion (B) and, in the sagittal plane,
toward the opposite ear. In effect, this puts the drill
virtually perpendicular to the skull. The ventricle is
entered with a cannula or ventriculostomy tube at
a depth of 7 to 8 cm (C). If the ventricle is not
entered in the first pass, two more passes can be
made, directed towards the ipsilateral and contra-
lateral pupil, respectively, instead of the nasion. If
three passes on each side do not result in success-
ful cannulation, the procedure should be aban-
doned.
Most dangerous traumatic unilateral intracranial
mass lesions will shift the midline 5 mm or more. This
will invariably be associated with an elevated ICP unless
a CSF leak is present. Significant temporal lobe lesions
may cause only a minimal shift of the midline, but the
ICP will usually be elevated and the third ventricle, if
seen, will often be shifted more than the lateral ventri-
cles. If there is little or no midline shift, the ICP is ele-
vated, and the patient is not hypercarbic, then there are
either bilateral mass lesions or serious diffuse brain in-
jury. A CT scan would resolve the issue, but when this is
not available the patient may have an angiogram per-
formed promptly to rule out bilateral "balancing" hema-
tomas or contusions that might require operative inter-
vention.
Twist-Drill Trephination
Mahoney and associates have reported their experi-
ence with emergency twist-drill trephination in the ER
in patients with a rapidly progressing uncal herniation
syndrome despite maximal medical therapy (58). This
can be used when there is any delay in obtaining a CT
scan, although we prefer to use an air ventriculogram. In
this study, 51 trephinations were performed in 41 pa-

252 / CHAPTER 12
tients with an 81 percent accuracy rate for the presence
or absence of a hematoma. The trephination was per-
formed on the side of the dilating pupil, two finger-
breadths above the zygomatic arch and two finger-
breadths anterior to the ear, using a ^f-inch diameter
hand drill. The dura was opened, and partial evacuation
of the hematoma was attempted by gentle suction. An-
drews and colleagues also made a case for exploratory
burr holes in patients with clinical signs of tentorial her-
niation or upper brainstem dysfunction on admission to
the emergency room (59). A hundred such patients were
taken directly to the operating room after intubation and
resuscitation, and sequential burr holes were made. A
complete exploration consisted of temporal, frontal, and
parietal holes. An extracerebral mass was found in 56 of
100 patients. In 38 patients, the exploration was negative
and the postoperative CT showed no significant hema-
toma. In six patients, an extra-axial hematoma that re-
quired surgery was missed. This option can be consid-
ered when a CT scan is not immediately available or
when the patient is clearly herniating.
Angiography
Indications. Angiography is undertaken in the
acutely head-injured patient when CT scanning is not
available. When CT scanning is available, angiography is
occasionally indicated as, for example, when a mass ef-
fect is seen on CT scan but no hematomas can be visual-
ized (the differential diagnosis includes an isodense he-
matoma and acute parenchymal swelling), when
vascular injury is suspected, or when the findings on CT
are not consistent with the patient's neurological status.
In a recent report of 24 patients with traumatic carotid
artery dissection, the presenting signs included Horner's
syndrome, dysphasia, hemiparesis, obtundation, and
monoparesis (60). When an isodense subdural hema-
toma is suspected, its presence can be confirmed by al-
tering the CT window setting or by using a contrast-en-
hanced study, prior to resorting to angiography.
Technique. Apart from the time involved in setting
up for angiography, this investigation requires a certain
degree of expertise in order to be performed safely and
effectively. When performed by experts, transfemoral
catheterization is the procedure of choice. It provides the
most information, but because it takes longer to set up
and is technically more difficult, it is not widely used for
head-injured patients. Angiograms are obtained in most
emergency rooms by direct injections into the common
carotid artery or internal carotid artery. In either case,
care must be taken to avoid entering the region of the
bifurcation, thus avoiding the carotid sinus and any ath-
eromatous plaques. An 18-gauge needle is used for this
procedure. The left hand anchors the carotid artery in
place against the vertebral bodies using the index and
middle fingers. The angiography needle is then inserted
between the two anchoring fingers and brought to lie
against the vessel wall. The wall of the vessel may also be
penetrated at right angles to minimize slippage and then
the needle brought into a plane parallel to the vessel into
which it is threaded. A 20-ml syringe with a stopcock and
connector tube is filled with saline and kept ready. A
nonionic water-soluble iodinated contract medium (e.g.,
Omnipaque 300) is drawn up in a 10-ml syringe and also
connected to the stopcock. Once the connector tubing is
connected to the needle, good blood flow is confirmed
with the saline syringe. The stopcock is then turned and
the contrast medium injected rapidly. Just before the
syringe is emptied, the technician begins shooting the
films. Biplane angiography with an automatic changer is
the ideal. However, when these are not available three
AP and three lateral films usually provide almost as
much data. Cross-filling of the opposite side may be facil-
itated by compression of the contralateral common ca-
rotid artery during injection of the contrast material.
The Seldinger technique may also be used for carotid
catheterizations. This involves penetrating the common
carotid artery low in the neck with an 18-gauge needle
and introducing a 50-cm long Seldinger guide through
the needle. The needle is then withdrawn when the guide
is 3 cm beyond its tip. A 30-cm catheter (PE 160) is then
introduced over the guide and, with a twisting motion, is
pushed into the vessel. The guide is then withdrawn.
Good blood flow should be obtained before contrast is
injected. If carotid dissection is suspected, a transfemoral
study should be obtained, because a direct carotid injec-
tion runs the risk of propagating the false lumen.
Interpretation. Supratentorial mass lesions usually
cause a contralateral shift of the anterior cerebral artery
and the internal cerebral vein [Fig. 8 (A) and (B)]. The
latter, being closer to the midpoint of the cranium, is less
affected by rotation of the film—a common problem
owing to rotation of the head to either side (61). Al-
though displacement of the vessels does not provide any
differentiating features between parenchymal swelling
and hematomas, a study of the pattern can help localize
the lesion. Frontal lesions cause a bowing of the anterior
cerebral artery, the so-called "rounded shift," with lim-
ited displacement, if any, of the internal cerebral vein.
Parietal lesions tend to cause a "square shift" of the ante-
rior cerebral artery primarily because of widening of the
unyielding falx cerebri posteriorly, and the internal cere-
bral vein is more markedly displaced. Temporal lobe le-
sions result in medial displacement of the internal ca-
rotid artery bifurcation and a characteristic upward
displacement of the middle cerebral artery group. This
may also be seen on the lateral views, but this is less
reliable because even mild rotation of the head can pro-
ject as an apparent upward bowing. It should be remem-
bered that parietooccipital lesions may not cause any
apparent shift of the midline as bilateral mass lesions
may balance each other [Fig. 8 (C)].
Infratentorial mass lesions are difficult to detect angio-
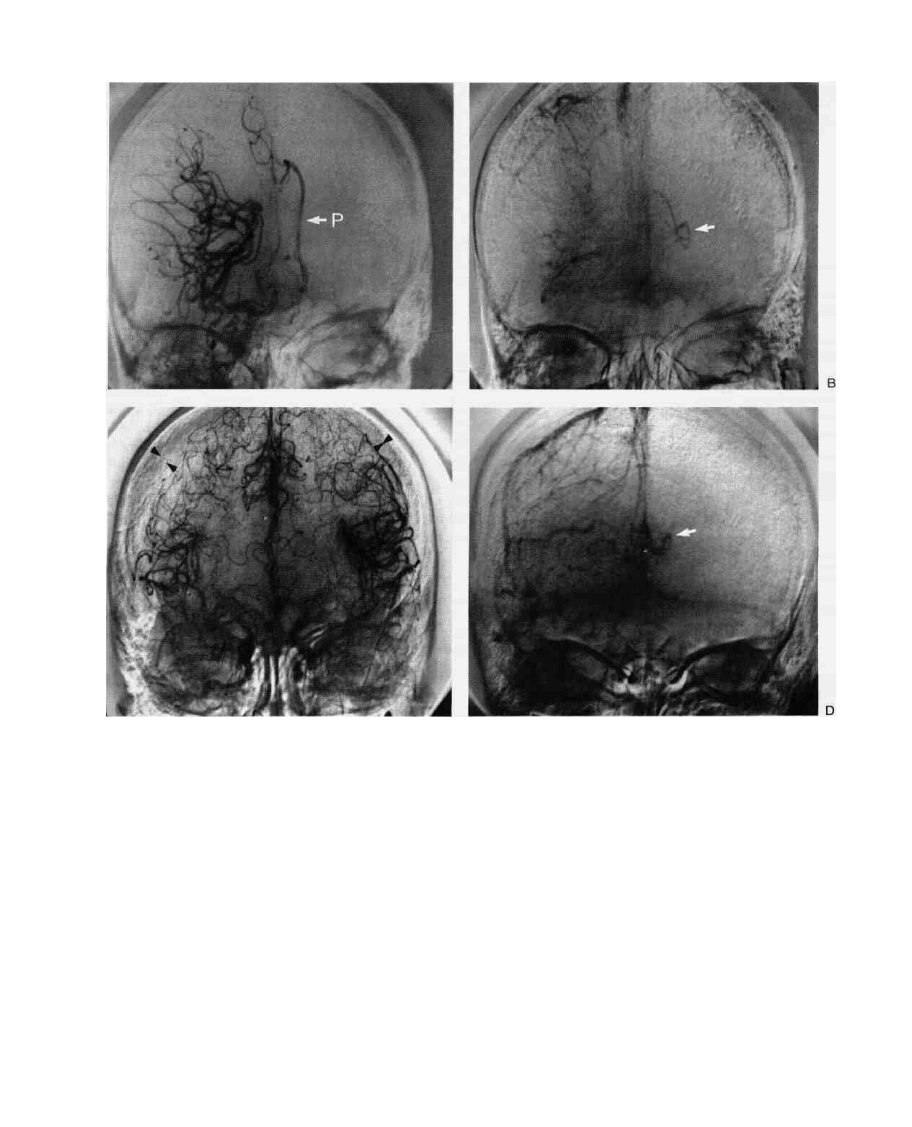
HEAD INJURY / 253
c
FIG. 8. Angiographic findings in head injury: (A) Acute right subdural hematoma, arterial phase. Note
that the midline cerebral artery branches are displaced away from the ,nner table of the skull and that UK;
sylvian point(s) is displaced toward the midline. The pericallosal artery (P) is markedly shifted across the
midline due to subfalcine herniation of the cingulate gyrus. (B) The venous phase of the same study
demonstrates a 2-cm right-to-left shift of the internal cerebral vein (arrow). Because this structure is
close to the center of the skull, rotation of the skull affects the pericallosal artery more than it affects this
structure. The internal cerebral vein is a paired midline structure, so the medial side of the vein represents
the midline. (C) Balancing bilateral hematomas. In the absence of midline shift on the angiogram as well
as on CT scan, bilateral hematomas should be suspected. Features suggestive of this diagnosis include
(1) inexplicably poor neurological state; (2) high ICP without obvious cause; and (3) subdural avascular
mantles. In this patient with bilateral subdural hematomas, note the crescentic avascular mantles—15
mm on the right and 1 0 mm on the left—with midline anterior cerebral arteries. (D) The shape of the
radiolucent mantle and other angiographic features are often not very helpful in distinguishing between
subdural and epidural hematomas. This patient was found to have both on the right side. Again, note the
dramatic shift of the internal cerebral vein to the left.
graphically, and vertebral injections are rarely under-
taken for this purpose. A posterior fossa mass may be
suspected if there is evidence of hydrocephalus on the
carotid films (i.e., upward sweep of the pericallosal artery
on the lateral film and a lateral bowing of the thalamo-
striate vessels on the anteroposterior films).
Transtentorial herniation is seen on anteroposterior
and lateral carotid angiograms as marked stretching of
the anterior choroidal artery as a result of medial uncal
displacement. If the posterior communicating arteries
are visualized, these will also be seen to be stretched and
sometimes compressed against the posterior clinoid pro-

254 CHAPTER 12
cesses. The posterior cerebral arteries are inferiorly dis-
placed on lateral view and are seen to be medially dis-
placed along with both superior cerebellar arteries on
anteroposterior view because of hippocampal gyrus her-
niation.
Mass lesions themselves usually present as avascular
areas on angiography. The classical appearance of an ex-
tra-axial hcmatoma on the AP view consists of a clear
gap between the inner table of the skull and the small
vessels on the surface of the brain as seen in the venous
phase [Fig. 8 (D)]. When the clot is located closer to the
vertex, oblique views may be needed to demonstrate its
presence, although displacement of a venous sinus away
from the bone may be seen on lateral views in certain
cases when the clot reaches the vertex. Subfrontal clots
may be suspected when the proximal anterior cerebral
artery is displaced upward and backward. Distinguishing
between extradural and subdural hematomas on an an-
giogram is an unreliable and somewhat academic exer-
cise [Fig. 8 (D)]. Abnormalities in transit time, spasm of
the intracranial vessels, and other forms of vascular in-
jury may also be seen in patients with head injury.
Computed Tomography
Indications. CT scanning is clearly the procedure of
choice in the evaluation of the head-injured patient and
has probably significantly improved outcome from head
injury (62). With every new generation of scanners, the
quality of information obtained is further enhanced.
However, most important decisions relating to patient
management are based on certain basic findings. It is
strongly recommended that an emergency CT scan be
obtained as soon as possible (preferably within half an
hour) after admission of a patient with a severe head
injury. Centers dealing with such patients must make
arrangements to have CT technicians in the hospital on a
24-hour basis or within easy accessibility in an emer-
gency. We also recommend repeat CT scans whenever
there is a change in the patient's clinical status or an
unexplained rise in intracranial pressure. Furthermore,
CT scan findings can be valuable in selecting patients for
ICP monitoring (30).
Technique. As soon as the patient's pulmonary status
is stabilized, the patient is rushed to the CT suite. At this
time, the operating room is warned of the possibility of a
craniotomy, and other steps are taken to ensure the p a -
tient's readiness for surgery, should it be necessary.
These include typing and cross-matching blood and con-
tacting relatives in order to obtain the necessary consent
for surgery. The patient is accompanied to the CT suite
by a physician because these patients are acutely ill and
often deteriorate suddenly. They are usually already in-
tubated. paralyzed, and on mechanical ventilation when
they reach the CT suite. It is unwise to become compla-
cent at this time, and frequent monitoring of vital signs
and pupillary reactions is strongly recommended.
If the scans reveal the presence of an operable mass
lesion, the patient is rushed to the operating room. Ma-
nipulating the scanner "window" during scanning is
sometimes useful in visualizing relatively isodense he-
matomas.
Interpretation. In a prospective study of CT scan ab-
normalities in 207 severely head-injured patients, we
found the initial CT scan to be normal in 30 percent of
cases. The remaining 70 percent of patients had CT scan
abnormalities: low-density lesions in 10 percent, high-
density nonsurgical lesions in 19 percent, and high-den-
sity lesions requiring surgery in 41 percent (30). Low-
density lesions, when seen in the absence of high-density
lesions, were interpreted as representing edema or in-
farction. Nonsurgical high-density lesions were contu-
sions or hematomas causing less than 5 mm of actual
midline shift. High-density lesions (epidural, subdural,
or intracerebral hematomas) were deemed to require
surgical decompression if they caused a midline shift
greater than 5 mm. In other words, considerable empha-
sis is placed on the degree of midline shift in deciding
which patients need surgical decompression. The signifi-
cance of midline shift in head-injury patients has been
examined by other authors, and some interesting cor-
relations with the level of consciousness have been
noted (63).
CT densities are measured by a scale first introduced
by Hounsfield (64) and subsequently modified by a fac-
tor of two. In this scale, water's absorption coefficient
(Hounsfield, or H, number) is 0, air's is -1000, and
bone's is +1000. The H numbers for intracranial struc-
tures are approximately as follows:
Air
Fat
Water
CSF
White matter
Gray matter
Extravasated blood
Bone or calcification
-1000
-100
0
4-10
22-36
32-46
50-90
800-1000
On CT, edema is seen as a zone of low density with
attenuation values ranging between 16 and 24 H, as
compared to white-matter values of 22 to 36 H. Asso-
ciated with this low density, a mass effect on the adjacent
ventricles may be seen, reflected as compression, distor-
tion, and displacement of the ventricular system. The
edema may be focal, multifocal, or diffuse. With diffuse
cerebral edema, it may be hard to appreciate the lower
density because no area of normal brain density is avail-
able for comparison [Fig. 9 (A)]. In such cases there is
usually bilateral ventricular compression, which may be
so gross as to result in nonvisualization of the ventricular
system, especially in children. It is debated as to whether
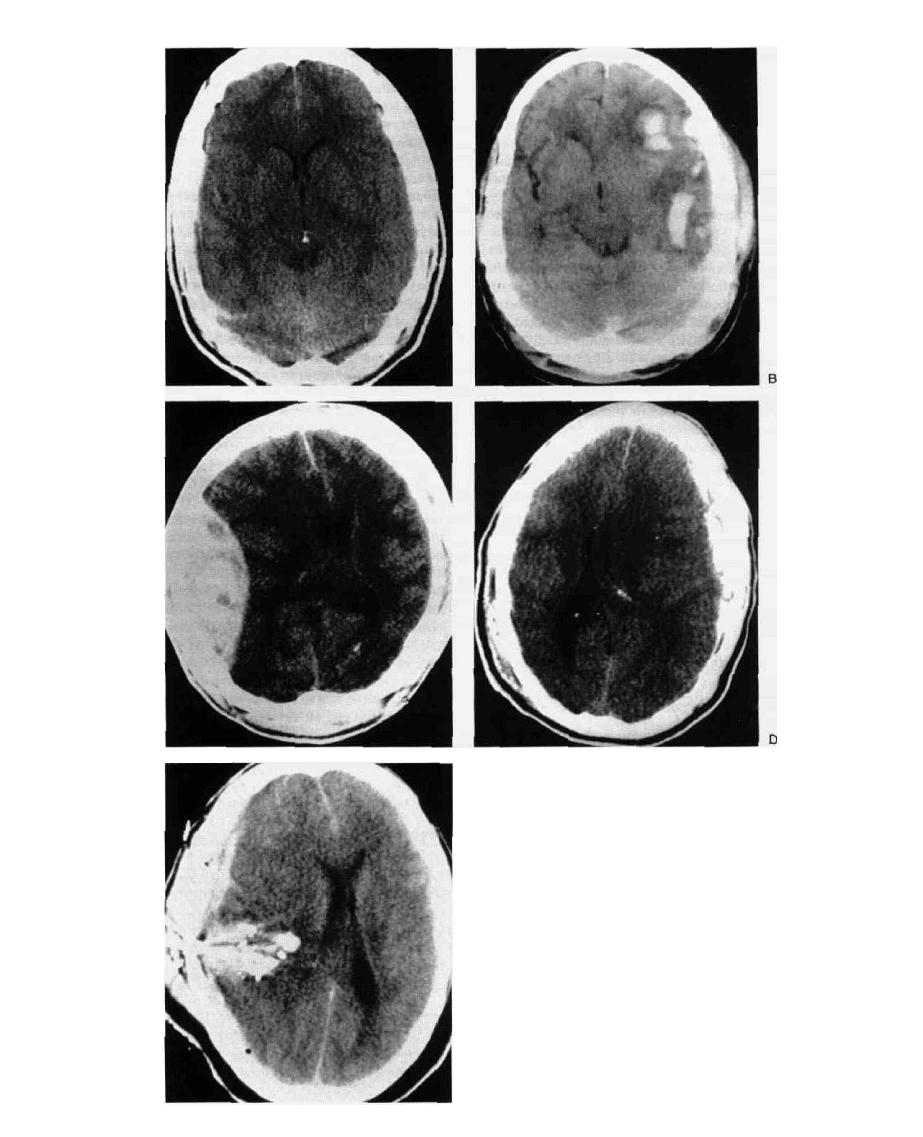
FIG. 9. CT findings in head injury: (A) Low-den-
sity lesions. These may be focal or, as in this ex-
ample, generalized. Note the almost complete
disappearance of the ventricles. (B) Contusions.
These are characterized by multiple small areas
of hemorrhage within the brain parenchyma, as-
sociated with surrounding areas of edema, and
result in the typical "salt-and-pepper" appear-
ance. (C) Subdural hematoma. Note that the hy-
perdense collection covers almost the entire sur-
face of the hemisphere and has a concave inner
margin. There is a 1-cm left-to-right shift of the
midline. (D) Epidural hematoma. This biconvex or
lenticular shape typifies an epidural hematoma.
Note the massive shift of the midline. (E) Gunshot
wound.
256 / CHAPTER 12
the picture of diffuse brain swelling is secondary to
edema or vascular engorgement. Although the attenua-
tion numbers could be expected to differentiate between
the two states, the issue is complicated by changes in
brain lipids after trauma (65). Miller and Corales con-
cluded that the concept of posttraumatic brain edema
has been overemphasized, and they emphasize the role
of vascular changes in the genesis of this morphological
picture (66).
Cerebral contusions are seen as nonhomogenous areas
of high density often interspersed with areas of low den-
sity, with attenuation values in the range of 50 to 60 H.
The CT appearance results from multiple small areas of
hemorrhage within the brain substance, associated with
areas of edema [Fig. 9 (B)]. The margin is usually poorly
denned. A mass effect is often seen, although this may be
minimal. Depending on the extent of hemorrhage, the
degree of edema, and the time course, a contusion may
appear predominantly dense or lucent. The outcomes
for patients demonstrating either low-density lesions or
nonsurgical high-density lesions (contusions) are very
similar, further suggesting that these morphological enti-
ties are closely related (Table 8).
Although it is not always possible to differentiate be-
tween subdural and epidural hematomas on CT, the lat-
ter are typically biconvex or lenticular in shape, because
the close attachment of the dura to the inner table of the
skull prevents the hematoma from spreading [Fig. 9 (C)].
Approximately 20 percent of patients with an extracere-
bral hematoma have blood in both the epidural and sub-
dural spaces at operation or autopsy (67). There is little
chance of epidural blood mixing with CSF, so these le-
sions appear as uniformly dense collections and are
rarely isodense. However, they may develop in a delayed
fashion, especially after evacuation of a contralateral
"balancing" lesion.
The typical subdural hematoma tends to be more dif-
fuse than an epidural hematoma and has a concave inner
margin that follows the surface of the brain [Fig. 9 (D)].
The distinction between acute, subacute, and chronic
lesions is somewhat arbitrary. However, in a study of 42
patients who were classified as acute if symptomatic for 0
to 7 days, subacute if symptomatic for 7 to 22 days, and
chronic if symptomatic for over 20 days, 100 percent of
the acute group had hyperdense lesions, 70 percent of the
subacute group had isodense lesions, and 76 percent of
the chronic group had hypodense lesions (68). Efface-
ment of the cerebral sulci over the convexity and distor-
tion of the ipsilateral lateral ventricle may serve as clues
that suggest the presence of an isodense hematoma. As
always, the degree of midline shift serves as the primary
criterion upon which decisions relating to surgical evacu-
ation of the hematoma are based.
Traumatic intracerebral hematomas are usually lo-
cated in the frontal and anterior temporal lobes, al-
though they may occur in virtually any area. The major-
ity of hematomas develop immediately after the injury,
but delayed lesions are not uncommon, usually develop-
ing within ihe first week. They are high-density lesions
with attenuation values of 70 to 90 H and are usually
surrounded by zones of low density caused by edema.
Traumatic hematomas are more often multiple than he-
matomas from other causes.
Intraventricular hemorrhage was previously believed
to have uniformly poor prognostic implications. This is
no longer considered true after the advent of CT scan-
ning (69). It is frequently associated with parenchymal
hemorrhage. The blood becomes isodense relatively rap-
idly and often disappears completely within a week. A
ventriculostomy is placed in the less bloody ventricle,
and a larger tube (No. 8 French) is used when intraven-
tricular blood is noted on CT.
Acute obstructive hydrocephalus may develop second-
ary to a posterior fossa hematoma that obstructs the ven-
tricular pathways. However, delayed hydrocephalus is
far more common, occurring in one study in 3 out of 48
patients with severe head injury who were followed with
serial CT scans (70). This communicating hydrocepha-
TABLE 8. Admission CT findings and outcome"
Outcome (%)"
CT group"
Normal
Low-density lesions only
High-density nonsurgical lesions
High-density surgical lesions
Total
# Cases
61
20
40
86
207
%
30
10
19
41
100
G
c
62
50
40
26
42
MD
d
18
10
20
•13 e,
15
SD/V
9
2
15
17
9
9
Dead
18
25
23
52
34
" From reference 30, with permission.
b
The correlation between CT (computed tomography) findings and outcome is significant (p < 0.0001). The difference in
outcome between normal and abnormal (low- or high-density lesions) CT scans is also significant (p < 0.0001).
0
G = good recovery
" MD - moderately disabled
8
SD = severely disabled; V = vegetative

HEAD INJURY / 257
lus results from blood in the subarachnoid space and is
usually evident by the 14th day post-injury. This entity is
discussed in greater detail later in this chapter.
Acute ischemic infarction appears as a low-density
area compared with the adjacent brain. The infarction
may be detectable on CT scan within 24 hours of onset,
and over 60 percent are clearly seen by seven days (71).
Contrast enhancement improves the diagnostic yield by
nearly 15 percent (72), and magnetic resonance imaging
(MRI) may be even more sensitive.
Indications for Surgery
It is difficult to lay down hard and fast rules regarding
the management of a disease as diverse as head injury.
However, we have arrived at certain guidelines that have
proven to be useful "in the trenches." Some of these
practices are based on hard data, some on clinical preju-
dice, and some on an irresistible desire to simplify a hope-
lessly complicated problem.
In its simplest form, our criterion for considering a
mass lesion operable is a midline shift of 5 mm or more.
Such a shift may be demonstrated by CT scan, angiogra-
phy, or ventriculography. Virtually all epidural, sub-
dural, or intracerebral hematomas associated with a
midline shift of 5 mm or more are surgically evacuated.
Occasionally one encounters a patient with a small he-
matoma with minimal shift who is alert and neurologi-
cally intact. A conservative approach is justified in such
cases, but the patient may deteriorate, ,and very close
observation is critical. Should there be any change in
mental status, a repeat CT scan should be obtained im-
mediately.
It is our policy to operate on all patients with an intra-
cranial mass lesion and 5-mm or more midline shift un-
less they are brain-dead. This policy is based on evidence
that some patients with bilaterally nonreactive pupils,
impaired oculocephalic responses, and decerebrate pos-
turing can nevertheless make a good recovery. In one
series, 3 of 19 such patients who were treated maximally
ended up in the "good" or "moderately disabled" cate-
gory, despite their foreboding constellation of signs (73).
The management of brain contusions is somewhat less
clear-cut. The only study that provided some guidance
in this area previously was that by Galbraith and Teas-
dale (74). In their series of 26 patients with acute trau-
matic intracranial hematomas who were managed with-
out surgery, they found that all patients with an ICP
greater than 30 mm Hg eventually deteriorated and re-
quired surgery. In contrast, only one patient with ICP
levels of less than 20 mm Hg deteriorated. Patients in the
20- to 30-mm Hg range were about evenly divided be-
tween the surgical and nonsurgical groups.
We have recently analyzed our experience with 130
head-injured patients with pure contusions who were
managed with CT scanning and, as needed, ICP moni-
toring in a neurosurgical intensive care unit (NICU) set-
ting (75). This study showed that patients with brain
contusions who could follow commands at admission
did not require ICP monitoring and as a rule did well
with simple observation. However, those who could not
follow commands (in the absence of a focal lesion in the
speech area) often had intracranial hypertension and de-
served to have their ICP monitored. The majority of
these patients who had compressed basal cisterns re-
quired surgery. We have found this algorithm to be very
useful in managing these patients.
It has been conclusively demonstrated that patients
with a large (over 30 cc) temporal lobe hematoma have a
much greater risk of developing tentorial herniation
than those with a frontal or parietooccipital lesion (76).
The bias should therefore tilt toward early surgery in
such cases.
When CT scanning is not immediately available, deci-
sions regarding surgery must be based on air ventricu-
lography and ICP measurements. Here again, a midline
shift of 5 mm or more indicates a need for immediate
surgical decompression. If there is no midline shift but
the ICP is elevated above 20 mm Hg, angiography
should be performed promptly to rule out bilateral bal-
ancing lesions.
When angiography is undertaken in patients with se-
vere head injury, the following findings should be consid-
ered as indications for an operation:
1. An intra- or extra-axial mass lesion causing a shift of
the anterior cerebral vessels across the midline to an
extent of 5 mm or more.
2. An extra-axial mass lesion more than 5 mm from the
inner table, if it is associated with any degree of ante-
rior or middle cerebral artery displacement.
3. Bilateral extra-axial mass lesions more than 5 mm
from the inner table. Except for patients who have
marked brain atrophy, such intracranial masses will
usually cause major elevations of ICP.
4. A temporal lobe intra-axial mass lesion causing a ma-
jor elevation of the middle cerebral artery or any de-
gree of midline shift. These patients are in a most
precarious position, because only slight swelling can
cause a tentorial herniation syndrome that progresses
very rapidly.
If the patient is considered a surgical candidate, he or
she is promptly moved to the operating room; if not, the
patient is moved to the NICU. If the patient is harboring
a mass lesion, mannitol (1 to 2 g/kg) should be adminis-
tered en route to the operating room. In addition, the
patient should be hyperventilated to achieve an arterial
Pco
2
of 25 to 30 mm Hg. As in all the maneuvers under-
taken thus far, time is of the essence. The sooner the
mass lesion is evacuated, the better the possibility of a
good recovery (17). If, on the other hand, no surgical

258 / CHAPTER 12
lesion is found, the patient is carefully monitored in the
NICU, both clinically and with various physiological pa-
rameters, notably ICP recordings and serial CT scans.
Any rise in ICP above 20 mm Hg that cannot be readily
explained and reversed and any deterioration in neuro-
logical status warrant prompt repetition of the CT scan
followed by the appropriate corrective measures.
SURGICAL CONSIDERATIONS
Anesthesia
The principal consideration in the selection of an anes-
thetic agent, or combination of agents, is the effect on
intracranial pressure. Because any agent that causes cere-
bral vasodilatation is likely to cause an increase in intra-
cranial pressure, such agents are to be avoided whenever
possible. One of the worst offenders in this regard is keta-
mine, which is a powerful cerebral vasodilator and is,
therefore, generally avoided in the head-injured patient.
All inhalation anesthetic agents can increase cerebral
blood flow to a lesser or greater extent. Volatile inhala-
tion agents, such as halothane, enflurane, and isoflurane,
can all increase cerebral blood flow, but they are proba-
bly safe in low concentrations. Isoflurane is the least
likely of these to cause cerebral vasodilatation. Nitrous
oxide has a slight vasodilatory effect that is probably
clinically insignificant, and it is therefore considered a
good agent for use in the head-injured patient. A com-
monly used combination is nitrous oxide (50 to 70 per-
cent with oxygen), an intravenous muscle relaxant, and
thiopental. The use of hyperventilation and mannitol
prior to and during induction can blunt the vasodilatory
effect and limit intracranial hypertension to some degree
while the cranium is being opened. If, during surgery,
malignant brain swelling occurs that is refractory to hy-
perventilation and mannitol, thiopental (Pentothal®) in
large doses (5 to 10 mg/kg) should be used. This agent
can cause hypotension, especially in a hypovolemic pa-
tient, and should therefore be used cautiously. As a last
resort, the use of judicious hypotension, with trimetha-
phan (Arfonad®) or nitroprusside (Nipride®) could be
considered. In such situations, it is important to rule out
other causes of brain swelling, such as venous congestion
from neck compression and the presence of an occult
hematoma either on the ipsilateral or the contralateral
side of the craniotomy.
Subdural Hematomas
Acute subdural hematomas may result from bleeding
from lacerated brain, bone cortical vessels, or an avulsed
bridging vein. Most of the obvious brain injury is seen in
the inferior frontal lobes and in the temporal lobes. In
order to be able to reach the midline, as well as the fron-
tal, temporal, and parietal regions, we advocate a large
flap for the treatment of acute subdural hematomas. The
scalp incision is a standard question mark beginning just
anterior to the tragus at the zygomatic arch, curving pos-
teriorly over the ear to the midline and then coming
down on the midline to a centimeter or so below the
hairline (Fig. 10). If the patient has been deteriorating
rapidly, a quick temporal decompression can be per-
formed via a small craniectomy, as shown in the figures.
This will reduce the pressure on the brainstem and could
possibly prevent or reverse tentorial herniation from oc-
curring. Once this has been achieved, the rest of the flap
can be completed. The medial extent of the craniotomy
should be approximately 1.5 cm off the midline in order
to avoid injury to the superior sagittal sinus or to one of
the venous lacunae or a draining vein. At the same time,
this flap opening permits the surgeon to visualize the
major draining veins easily and to be able to reach an
avulsed vein near the midline. The anterior extent of the
bone flap may be varied, depending on the extent of
frontal damage and blood clot seen on the CT scan. A
subtemporal craniectomy is useful as a pressure valve.
Indeed, it has been demonstrated that a large subtem-
poral craniectomy can make it easier to control intracra-
nial hypertension in situations where all other medical
means have failed (77). We routinely use the operative
ultrasound to rule out the presence of previously unde-
tected intracerebral hematomas or a growing mass lesion
on the opposite side of the brain (Fig. 11). The majority
of the patients with an acute subdural hematoma have
associated intracerebral contusions or hematomas.
Epidural Hematomas
Epidural hematomas are typically located in the tem-
poral region and often result from tearing of the middle
meningeal vessels secondary to a temporal bone frac-
ture. Venous epidural hematomas may occur as a result
of a skull fracture or an associated venous sinus injury.
They generally tend to be smaller and are associated with
a more benign course. These may, in certain cases, be
safely treated nonsurgically, especially when they pres-
ent to the neurosurgeon several hours after the initial
injury. However, most epidural hematomas represent a
surgical emergency and should be evacuated as rapidly
as possible. Because the brain underlying an acute epidu-
ral hematoma is generally fairly normal, every effort
should be made to relieve the pressure as soon as possible
to avert any brain damage. The outcome from surgery
for an epidural hematoma is very closely related to the
patient's clinical condition prior to surgical evacuation.
If the clot is large, or if there is any doubt as to the extent
of underlying brain damage, the standard large craniot-
omy flap is recommended. In instances where the epidu-
ral hematoma is clearly localized to one region and there
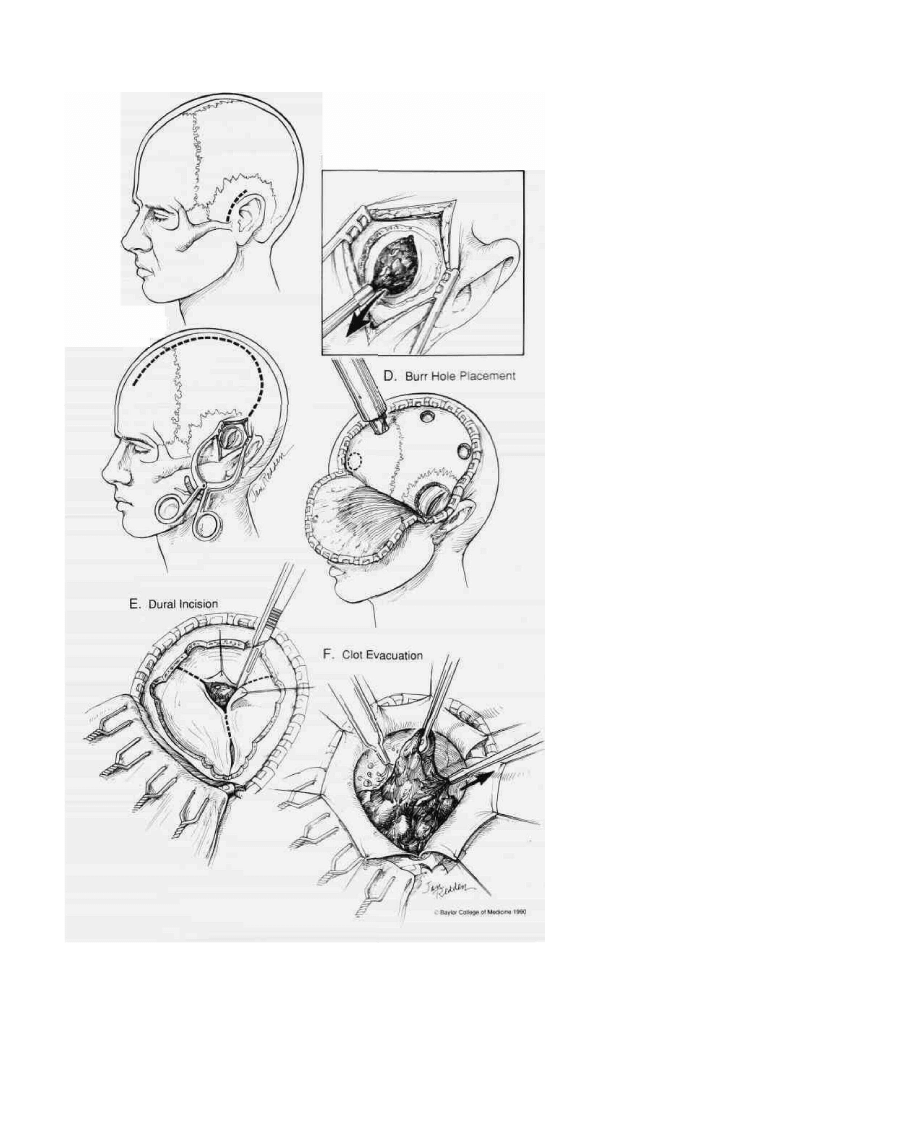
HEAD INJURY / 259
A. Initial Incision
C. Completed
Incision
B. Temporal Decompression
is no associated subdural blood seen on the CT scan, a
smaller modified craniotomy flap may be used.
Intracerebral Hematomas
Brain injury is often an evolving phenomenon. The
CT scan at admission frequently deteriorates over the
FIG. 10. Evacuation of an acute subdural he-
matoma: (A) In instances when there is evi-
dence of rapid neurological deterioration sec-
ondary to a herniation syndrome, temporal
decompression is recommended as the first
step. An incision is made just anterior to the
ear and taken down to the zygoma, which
marks the floor of the temporal fossa. (B) A
burr hole is made, followed by a quick craniec-
tomy. The dura is incised and as much of the
blood clot as possible is aspirated. (C) The in-
cision is then extended upwards to form a
large question mark, the medial extent of
which follows the midline. (D) Additional burr
holes are then made, with the medial ones 1.5
cm off the midline to avoid injury to the major
venous structures and granulations. The ante-
rior burr hole is placed above the frontal sinus,
the size of which can be estimated from preop-
erative radiographs. (E) The dura can be
opened with a Y-shaped or X-shaped incision,
with a flap being based on the superior sagit-
tal sinus. (F) The subdural hematoma is gently
evacuated with suction, irrigation, and other
mechanical means. Sources of bleeding are
identified and cauterized. Contused brain is
debrided, and pial edges are carefully cauter-
ized. The ultrasound is used to rule out the
presence of occult intracerebral or contralat-
eral hematomas.
next several days, resulting in what have come to be
known as delayed traumatic intracerebral hematomas
(DTICHs) (Fig. 12). This interesting clinical phenome-
non of uncertain pathogenesis and debatable prognostic
significance has been discussed by several authors (78-
84). Contusions are most often located on the anterior
and inferior surfaces of the frontal and temporal lobes.
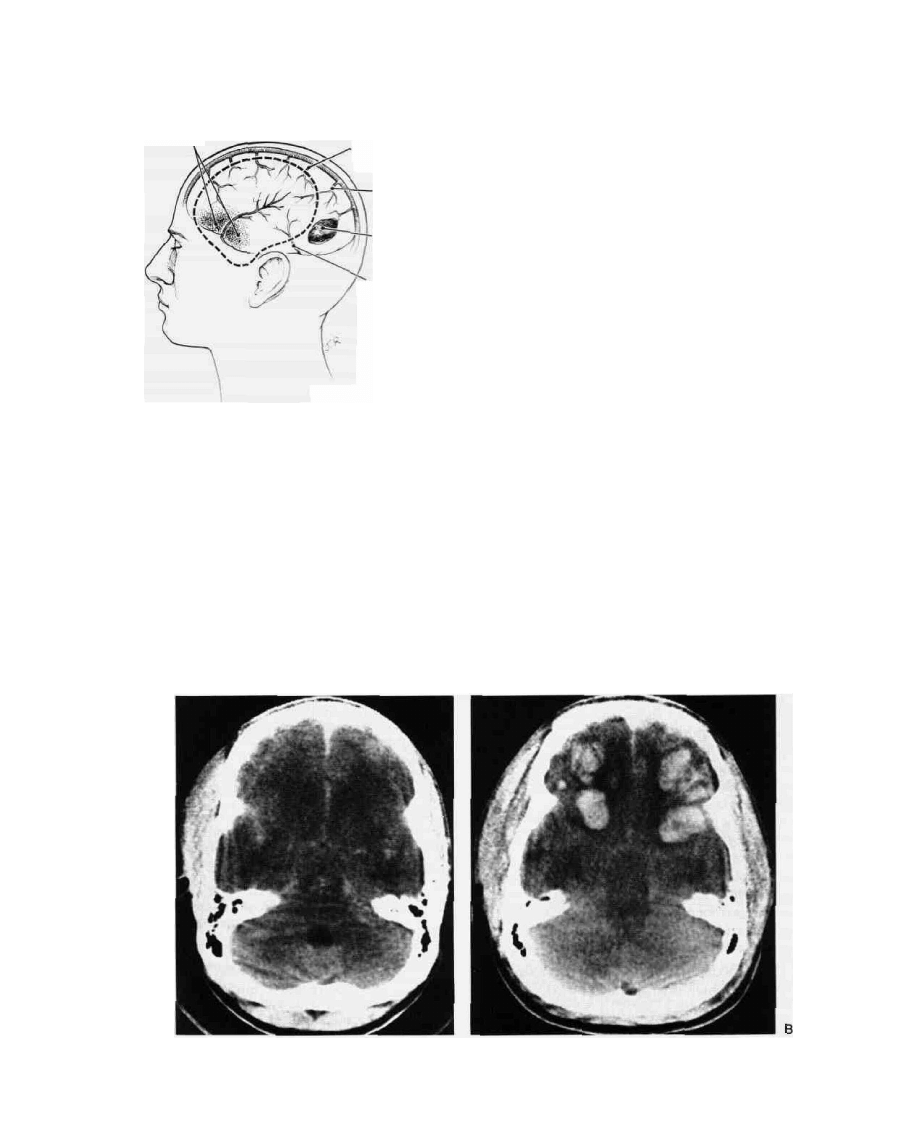
260 / CHAPTER 12
Debride frontal and
temporal contusions
Observe brain swelling and
rule out intracerebral and
contralateral hematomas
with ultrasonography
Look for bleeding from
draining veins
Protect vein of Trolard
Look for residual hematomas
beyond limits of flap
Protect vein of Labbe
e Baytor Cotege of Medicine 1990
FIG. 1 1 . Precautions to be taken during a craniot-
omy for subdural hematoma.
Contusions measuring larger than approximately 2 cm
should generally be debrided if they are causing a signifi-
cant mass effect. Care should be taken to stay within
necrotic brain and to avoid damaging surrounding nor-
mal tissue. This distinction cannot always be easily made
and requires some nicety of clinical judgment. As a gen-
eral rule, debridement of the left temporal lobe is per-
formed more conservatively than debridement on the
right side, particularly in right-handed patients.
Posterior Fossa Hematomas
These are fortunately less common than supratentor-
ial lesions. In general, an aggressive surgical approach is
advocated in the management of these lesions, because
these patients can deteriorate very rapidly. A patient
with a posterior fossa hematoma could deteriorate from
a responsive state to a comatose condition within a mat-
ter of minutes. Furthermore, because it generally takes
FIG. 12. Delayed traumatic intracerebral hematomas: (A) Non-enhanced CT scan of a patient with a
severe head injury at admission. (B) Repeat study two days later shows extensive delayed traumatic
intracerebral hematomas in both frontal lobes.

HEAD INJURY / 261
FIG. 13. Depressed skull fracture. CT scan of a right parietal
depressed fracture showing the overlying scalp hematoma
that can mask the degree of depression. Note the obvious
compromise of the underlying brain tissue.
longer to evacuate such a lesion and because the brain
structures that are located in the posterior fossa are so
much more critical to the vital functions, the surgeon
does not have much leeway in terms of time. A prone or
three-quarter prone position with a Mayfield headholder
is generally used.
Depressed Fractures
A skull fracture is considered significantly depressed if
the outer table of the skull lies below the level of the
inner table of the surrounding bone. Sometimes such
depression may not be evident on plain x-rays, but it is
usually clearly seen on the CT scan (Fig. 13). Depressed
skull fractures can be either closed or compound. Most
closed depressed fractures occur in young children and
may be of the "ping pong ball" variety. The most com-
mon indication for surgery in such cases is cosmetic,
especially with frontal fractures. In compound depressed
fractures, the wounds are often dirty and contaminated.
Often skin, hair, or other foreign debris will be wedged
between the depressed bone fragments, even when the
wound looks relatively clean from the outside. There-
fore, except in the simplest of injuries, closing of such
fractures in the operating room is recommended. Often
a dural laceration underlies the fracture, and great care
should be taken to close this primarily. However, the
presence of an intact dura does not necessarily preclude
an underlying brain contusion. A preoperative CT scan
is therefore very useful in defining the extent of the sur-
gery required. It is generally considered acceptable to
replace bone fragments at the craniectomy site. The post-
operative infection rate with such replacement is re-
ported to be less than 5 percent (85). Depressed fractures
overlying major venous sinuses (Fig. 14) are harder to
treat. The issues relating to sinus injuries are briefly dis-
cussed in the next section.
Penetrating Head Injuries
In the United States, penetrating head injuries are
most commonly secondary to gunshot wounds. In the
civilian setting, these are overwhelmingly secondary to
handguns. The severity of the head injury can vary with
the caliber of the weapon, the distance from which it was
fired, the ammunition used, and the trajectory of the
FIG. 14. Depressed skull fracture overlying the superior
sagittal sinus. When dealing with such injuries, the sur-
geon must be prepared to deal with massive, sudden
blood loss. The anterior third of the sinus may be ligated,
but every effort should be made to repair the posterior
two-thirds.

262 / CHAPTER 12
bullet. Plain x-rays of the skull and a CT scan are invalu-
able in planning management in any given case. In the
military setting, high-velocity injuries from rifles are also
encountered, and these are certainly more devastating.
In addition, military wounds are often secondary to
shrapnel, which are usually of lower velocity because of
their irregular shape. Penetrating injuries can also be sec-
ondary to a variety of nonmissile objects, such as knives
or scissors, which cause local brain damage but little dif-
fuse "shock" injury.
The surgical approach to penetrating head injuries
(Fig. 15) is somewhat different than that used with closed
head injury. If a penetrating object is still in place and is
projecting out of the skull, it is left in place until the
patient is completely ready fo^ surgical intervention.
This is done to avoid torrential bleeding, which may en-
sue after removal of such an object. Unlike surgery for
closed head injury, surgery for penetrating head injuries
usually involves making a limited cranial opening. The
scalp opening may be just a linear or S-shaped extension
of the entrance wound or a limited U-shaped flap. The
opening into the cranium may be via a craniectomy, or,
if the surgeon prefers it, by a small craniotomy. The
main purpose of the surgery is to debride the necrotic
brain, remove bone fragments and other foreign bodies
from the brain parenchyma, arrest bleeding, evacuate
any hematoma, and finally to secure water-tight closure
of the dura and scalp. Often, bullet fragments have pene-
trated into the other side of the brain. Unless these are
easily accessible, surgery does not necessarily need to be
taken on the opposite side in order to remove the bullet.
It was standard Army policy to reoperate on patients
whose cranial gunshot wounds had been closed at front-
line hospitals, in order to remove all bone fragments.
However, the Vietnam Head Injury Study demonstrated
by CT that the vast majority of such patients harbor
small bone fragments despite a second operation and do
not seem to demonstrate an increased incidence of com-
plications. Complete removal of such bone fragments is
not likely to be accomplished without sacrificing some
normal brain in the process. Therefore, it is now believed
that a reasonable degree of debridement under antibiotic
cover is a safe and reasonable option (86). This has
been borne out by military experience in Lebanon as
well (87).
Venous Sinus Injuries
Venous sinus injuries are among the most difficult in-
juries a neurosurgeon has to face. Major sinuses can be
either ligatcd or reconstructed. It is generally true that
the anterior third of the superior sagittal sinus can be
safely ligated. but ligation of the posterior third is most
likely to produce massive venous infarction of the brain.
Ligation in the middle third has somewhat unpredict-
able effects, and ligation of the dominant transverse si-
nuses can also have disastrous effects. If an attempt is to
be made to repair a major venous sinus, the Kapp-Giel-
chinsky shunt can be a useful device (46). This is a typi-
cal vascular shunt, but it has inflatable balloons at both
ends. It can be used to maintain venous blood flow while
the reconstruction is being planned or executed. It is of-
ten technically easier to use dural flaps to oversew sinus
injuries. Other standard neurosurgical maneuvers using
pressure, gelfoam, Surgicel®, and other hemostatic
agents may be invaluable in controlling the bleeding.
The use of a rapid autotransfusion unit can limit the
amount of blood transfusions required, thus reducing
the pressures on the blood bank and minimizing the risk
of blood transfusions for the patient.
THERAPEUTIC AGENTS
Advances in the "intensivist" approach to acute ill-
ness have resulted in more scientific and thorough meth-
ods of managing head-injured patients, with their multi-
ple associated problems. Aggressive management of
such problems is, logically, likely to reduce the incidence
of secondary insults. One would expect that such an ap-
proach can reduce mortality owing to medical complica-
tions, and this has been the experience in well-docu-
mented prospective series (29,73,88,89). These studies
have also shown that the majority of patients "saved" by
such aggressive management do not join the ranks of the
severely disabled or vegetative but actually go on to be-
come only moderately disabled or to make a good recov-
ery. Thus, a systematic and intensive approach to the
management of severe head injury is effective enough to
justify the commitment of additional resources in this
direction (90).
Unfortunately, our experience with drug therapies has
so far been less than satisfactory. Owing to the irrevers-
ibility of some of the damage and to the complexity of
the pathogenesis of brain injury, it seems unlikely that a
penicillin-like wonder-drug will be found. It seems more
likely that a combination of several agents and interven-
tions, each with its small beneficial effect, will make a
significant cumulative impact on outcome. These small
effects of individual agents arc difficult to demonstrate
conclusively given the nonhomogeneity of head-injured
patients, the large number of patients required to com-
plete such clinical trials, and the prohibitive cost. With
this background in mind, we can briefly review the drugs
commonly in use and speculate upon other possibilities.
Anticonvulsants
The use of prophylactic anticonvulsants in patients
with severe head injury remains controversial (91 -98). A
survey of neurosurgeons in 1972 revealed that 40 per-
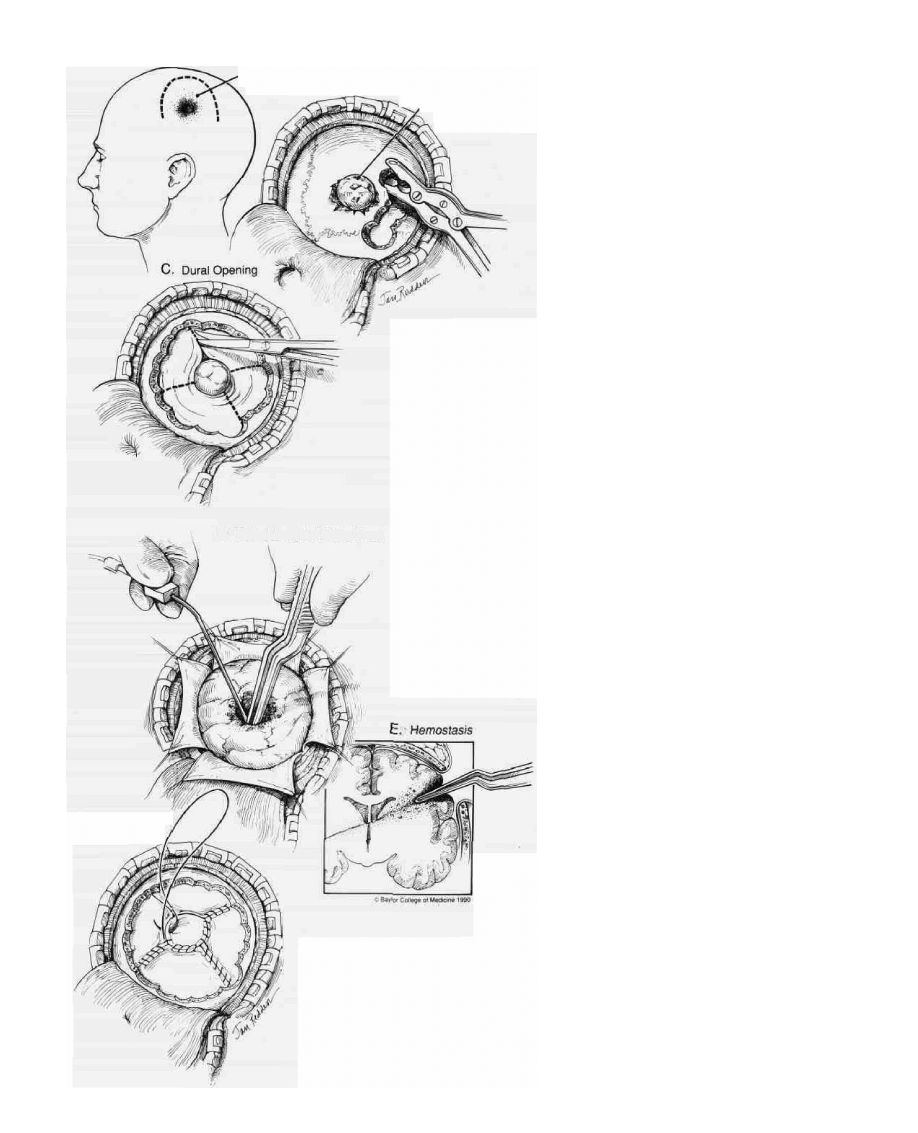
A. Small Scalp Flap
Powder burns in
'close-range injury
B. Craniectomy
, Bullet entry site
D. Debridement of Bullet Tract
F. Dural Closure
and Repair
FIG. 15. Surgery for penetrating head in-
jury. The approach to penetrating head inju-
ries is somewhat different from that for
closed head injuries because the damage
tends to be more focal. The entry and exit
sites are treated similarly. (A) A small linear
or S-shaped incision incorporating the entry
wound is recommended. (B) A craniectomy
is performed at the entry site in the skull. (C)
The dura is opened in a cruciate fashion. (D)
Blood, necrotic brain, bone and bullet frag-
ments along the path of injury are debrided.
(E) Hemostasis is secured with bipolar cau-
tery and hemostatic agents. (F) Dural repair
is completed using pericranium or lyophi-
lized dura as needed.

264 / CHAPTER 12
•cent of them did not use these drugs routinely either
-because they were uncertain of the indications or be-
cause the risk was considered too low to justify treatment
(93). Jennett conducted a major study of posttraumatic
epilepsy and found this complication to occur in about 5
percent of all patients admitted to the hospital with non-
missile head injuries and in 15 percent of those with se-
vere head injuries (91). Three main factors were found to
be linked to a high incidence of late epilepsy (Table 9);
(1) early seizures, occurring within the first week: (2) an
intracranial hematoma; and (3) a depressed skull frac-
ture. It has been suggested that prophylactic treatment
with phenytoin initiated as early as possible (within 24
hours) might prevent the development Of an epilepto-
genic focus. However. Young and associates" random-
ized, double-blind, placebo-controlled studies showed
that prophylactically administered phenytoin did not
prevent either early or late posttraumatic seizures (94-
96). In these studies, plasma concentrations were main-
tained between 10 and 20 jig/ml. Although the authors
caution that maintaining higher drug levels could have
altered the results of the study, they recommend using
anticonvulsants only after a patient has had a seizure.
McQueen and coworkers however, pointed out that be-
cause of the low incidence of posttraumatic seizures (7%
at one year; 10% at two years), randomized clinical trials
must include about 1200 patients to be conclusive (97).
If so, all reported trials have been too small (by a factor of
at least six). The weight of evidence therefore currently
supports the routine use of anticonvulsants in high-risk
groups (as denned above), but not necessarily in all pa-
tients with head injury. Temkin and associates recently
reported results from a double-blind study in which 404
severely head-injured patients randomly received phen-
ytoin or placebo beginning within 24 hours of injury and
continuing for one year (98). They found that phenytoin
reduced the incidence of seizures during the first week
after injury, but not thereafter.
Our present practice is to use phenytoin (500 mg intra-
venously over 10 minutes) in the emergency room in all
patients with severe head injury. Doses are adjusted to
achieve therapeutic blood levels. According to the find-
ings of Young and associates, aiming for blood levels
higher than 15 to 20 /ug/ml may be justified (95,96). The
entire requirement may be taken as a single daily dose
(99). There are no hard and fast rules for when to stop
anticonvulsants, although the recent Temkin study
TABLE 9. Main factors associated with late epilepsy
3
1 . No early epilepsy
Early epilepsy
2. No intracranial hematoma
Hematoma
3. No depressed fracture
Depressed fracture
3%
25%
3%
35%
3%
17%
' Adapted from reference 261, with permission.
would justify stopping treatment after the first week in
most cases (98). The EEG is not generally contributory
in making this decision. The drugs should be tapered off
gradually, rather than stopped abruptly (100). There is
some evidence to suggest that carbamazapine (Tegre-
tol®) may be preferable to phenytoin for long-term use
because of improved performance on tests of cognitive
function (101).
Steroids
Although corticosteroids have not been conclusively
shown to be effective in head injury, many neurosurg-
eons use them in severe cases. Two studies have sug-
gested that very large doses of steroids may reduce the
mortality rate in severe head injury (102,103). However,
closer examination of the study done by Faupel and as-
sociates reveals that the reported decrease in mortality
was achieved as a result of a large increase in the number
of vegetative survivors (102). If the outcome groups are
divided into good outcome (good recovery and moder-
ately disabled) and poor outcome (severely disabled, veg-
etative, and dead), there was no statistical difference be-
tween the steroid- and placebo-treated groups. Gobiet
and associates compared a high-dose dexamethasone
group (96 mg/day) with a conventional dose group (16
mg/day), and a placebo group. There was no statistical
difference in mortality between the high-dose and the
placebo group, but this study was limited by being non-
blinded and sequential (all patients in one year received
the same treatment) (103).
One must, however, beware of a type II error and of
missing actual beneficial effects because of inadequate
sample sizes (104). A study by Saul, Ducker, Salcman,
and Cairo suggests that steroids may help certain sub-
groups of patients with head injury (105). However, the
literature contains several articles in support of the view
that traumatic brain injuries, in contrast to brain tu-
mors, do not respond well to steroids, either in terms of
ICP control or in terms of improved outcome (106-
109). Most recently, the NASCISII study, which showed
a beneficial effect of very high-dose methylprednisolone
in spinal cord injury, may rekindle interest in the appli-
cation of steroids for head injury (110).
Mannitol
This agent is now widely employed to reduce intracra-
nial pressure. The commonly used preparation is a 20
percent solution of mannitol (mw 180). It has been gener-
ally believed that mannitol establishes an osmotic gra-
dient between the plasma and the brain, resulting in a
shift of water out of the brain and, therefore, in a fall in
ICP. Proving this has been somewhat difficult (111), how-
ever, and there certainly may be other mechanisms by

HEAD INJURY / 265
which mannitol lowers ICP (112-114). Serum osmolal-
ity should not be allowed to go above 320 osmoles/liter,
if possible, in order to avoid systemic acidosis and renal
failure (115). Views relating to the appropriate dose of
mannitol vary (116). The most widely accepted regimen'
is 1 to 2 g/kg given intravenously as quickly as possible.
If a patient shows evidence of neurological deterioration
or tentorial herniation, we administer mannitol rapidly
en route to the CT scanner. The patient should have a
Foley catheter in place at this point, as diuresis can be
expected. With continued use, intravascular mannitol
equilibrates with the brain and progressively higher
blood levels are required to elicit a response.
Thirty percent urea (mw 60) and 10 percent glycerol
(mw 92) were previously used interchangeably with
mannitol in the chronic setting. These agents have
smaller molecular weights and tend to equilibrate more
rapidly with the brain. Urea is also associated with a high
incidence of hemoglobinuria and severe sloughing of the
skin if it infiltrates (117). Wald and McLaurin have re-
ported on their experience with oral glycerol in head in-
jury patients (118). However, oral agents should not be
considered in the treatment of an acutely injured patient
for obvious reasons.
Lasix
Certain authors have reported the use of furosemide,
either alone or in conjunction with mannitol, in head
injury (119) and in other states. Schcttini, Stahurski, and
Young demonstrated that diuresis could be enhanced by
the combined use of mannitol and furosemide in neuro-
surgical patients, with more pronounced and consistent
brain shrinkage (120). In their study, a peak diuresis of
17 ml/min was reached within 30 minutes of mannitol
administration, with a fall to 4 ml/min during the next
70 minutes. By contrast, during an identical time course,
combined mannitol-furosemide infusion yielded an ini-
tial water excretion rate of 30 ml/min, followed by a
further increase to 42 ml/min, and then by a decline
to 17 ml/min. The patients were given 1.4 g/kg of man-
nitol ±0.3 mg/kg of furosemide. The only adverse effect
noted with combined therapy was accelerated electrolyte
loss, which had to be corrected. These findings were con-
firmed by Wilkinson and Rosenfeld (121).
Sodium Bicarbonate
Along with hypoxemia, a low arterial pH on admis-
sion, indicating systemic acidosis, is not uncommon. If
the patient has been in shock, this is usually lactic acido-
sis. If the arterial CO
2
tension (Paco
2
) is high, it indicates
a mixed respiratory and metabolic acidosis. The acidosis
should be corrected, and sodium bicarbonate may be
given in a dosage of 1 mEq/kg every 10 minutes or so
until it is resolved. It should, however, be remembered
that reversal of mild acidosis can occur quickly and spon-
taneously when ventilation and perfusion arc restored by
intubation and normalization of systemic arterial pres-
sure. As a general rule, an arterial blood pH under 7.1
indicates severe metabolic acidosis and calls for the use
of sodium bicarbonate. At this level, cardiac function is
adversely affected by the acidosis (122). The dosage may
be roughly estimated by the following formula: dosage of
sodium bicarbonate (mEq) equals 0.2 times the body
weight (kg) times 27 mEq/1 minus the patient's serum
bicarbonate level. Half the calculated dose is given ini-
tially, and subsequent doses are administered after re-
peat pH determinations.
When massive blood transfusions are given to patients
in severe shock, an ampule of sodium bicarbonate
(about 45 mEq) should probably be given with every two
to three units of whole blood in order to correct for the
acidity of banked blood.
Tris-hydroxy-methyl-aminomethane (THAM)
It has been demonstrated that brain injury is asso-
ciated with metabolic acidosis as reflected in high CSF
lactate levels (123.124). It has also been shown that pa-
tients with higher CSF lactate levels have a worse out-
come and that those with a deteriorating course gener-
ally show a progressive fall in CSF pH from 7.3 to 7.2
owing to lactic acidosis (125,126). Several groups have
examined the role of acidosis in the pathogenesis of neu-
ronal damage (127-129). DeSalles, Kontos, and Becker
recently studied the prognostic significance of ventricu-
lar CSF lactate in severe head injury (130) and noted
lower pH values in the brains of three patients who un-
derwent surgery for acute subdural hematomas (131).
THAM is a buffering agent that penetrates the CNS and,
therefore, is theoretically superior to sodium bicarbonate
for the treatment of CNS acidosis. Akioka and col-
leagues, using a dog epidural balloon model, demon-
strated a beneficial effect of THAM on ICP (132). This
was confirmed by Gaab and associates using a cold-le-
sion edema model in rats (133). Subsequently, Rosner
and Becker reported a beneficial effect of THAM in a cat
fluid percussion model (134). They found that THAM
was associated with reduced morbidity and mortality as
well as lowered ICP after percussion injury. A clinical
trial is now being conducted with this agent at the Medi-
cal College of Virginia (H.F. Young, personal communi-
cation).
Barbiturates
Several studies have demonstrated the protective ef-
fect of barbiturates on the brain in cerebral anoxia and
ischemia (135-137). It has also been documented that
barbiturates are effective in reducing intracranial pres-

266
/ CHAPTER 12
sure (135-139). However, two randomized prospective
studies—one from Richmond (140) and the other from
Toronto (141)—indicated that no benefit was derived
from high-dose barbiturates in terms of either ICP con-
trol or outcome. In both of these studies, barbiturates
were given as the initial therapy. In a recently completed
prospective randomized multicenter trial in which high-
dose pentobarbital was given after all conventional
means of ICP control had failed, a clearly beneficial ef-
fect was noted on ICP levels (142). Because of the study's
cross-over design, no conclusion could be made regard-
ing the effect of pentobarbital on outcome. However, it is
evident that barbiturates should be reserved for a small
subset of patients who have failed all other forms of ther-
apy for intracranial hypertension.
One protocol for pentobarbital therapy is to give a
loading dose of 10 mg/kg over 30 minutes and 5 mg/kg
every hour for three hours, followed by a maintenance
dose of 1 mg/kg/hr adjusted to achieve a serum level of 3
to 4 mg%. Hypotension is often a limiting factor.
Naloxone
Naloxone, the narcotic antagonist, has been shown to
reverse hypotension associated with head injury in cats
(143). It is conceivable that a release of endogenous
opiates may be responsible for this postconcussive hypo-
tension (144). Few data either support or refute the value
of this agent in head injury. The recent NASCISII study
showed no beneficial effect of naloxone in spinal cord
injury (110).
Short-Acting Hypnotics
Because of the tendency of barbiturates to cause hypo-
tension and to prolong recovery after cessation, there has
been a search for shorter-acting anesthetic agents to con-
trol intracranial hypertension. Althesin, an intravenous
steroidal anesthetic agent, although never approved for
use in the United States, was popular in Britain for a
while before its manufacture was discontinued because
of concerns relating to anaphylaxis (145). Etomidate ap-
pears to be a satisfactory alternative for anesthetic use,
but no data are available on long-term use in head-injury
patients (145).
Hyperbaric Oxygen
Although Sukoff and Ragatz reported in 1981 that hy-
perbanc oxygen therapy (HBO) can reduce ICP and may
be of value in the treatment of traumatic cerebral edema
(146). this therapeutic modality is not widely used be-
cause, in general, results have been less than impressive.
Furthermore, this treatment does call for investment in a
hyperbaric chamber and is labor-intensive when dealing
with critically ill patients. However, these authors did
demonstrate a consistent reduction in ICP during expo-
sure to hyperbaric oxygen at two atmospheres pressure
and reported neurological improvement. Recently,
Rockswold, Ford, Bergman, and Anderson reported the
results of their prospective randomized study of HBO in
severe head injury (147). They found that although HBO
significantly improved survival in patients with a GCS
score of 4 to 6, it did not improve the percentage of
patients making a good recovery.
Free Radical Scavengers
The role of oxygen radicals in the pathogenesis of head
injury has received much recent attention (148). Schet-
tini, Lippman, and Walsh demonstrated a dramatic re-
duction in mortality in a dog cpidural balloon compres-
sion-decompression model with the use of native
superoxide dismutase (SOD) after injury (149). Because
of this study and other experimental data, SOD in its
native as well as its conjugated form (PEG-SOD) is
currently undergoing early clinical testing.
INTRACRANIAL PRESSURE
MONITORING AND CONTROL
Several pathological processes that affect the brain can
cause elevation of intracranial pressure. In turn, intracra-
nial hypertension can have consequences that adversely
affect the patient's outcome. Thus, elevated ICP not only
indicates the presence of a problem but can often contrib-
ute to it. Continuous monitoring of ICP was pioneered
by Guillaume and Janny in 1951 (150) and was applied
systematically to head-injured patients by Lundberg in
1960 (151). Since the early 1970s, there has been increas-
ing interest in ICP monitoring and a progressive evolu-
tion of related technology. ICP monitoring is now selec-
tively applied to severely head-injured patients in
virtually all major neurosurgical centers in the United
States.
Basic Physiology
Normal ICP in the resting state is approximately 10
mm Hg (136 mm H
2
O). As a broad generalization, pres-
sures over 20 mm Hg are considered abnormal, and
pressures over 40 mm Hg can be categorized as severe
elevations. It has been clearly demonstrated that higher
ICP following head injury is associated with a poorer
outcome. CSF is formed mainly in the choroid plexuses
of the lateral and third ventricles, and the daily produc-
tion of CSF is approximately 500 ml. Approximately
150 ml of CSF is present within the craniospinal axis.
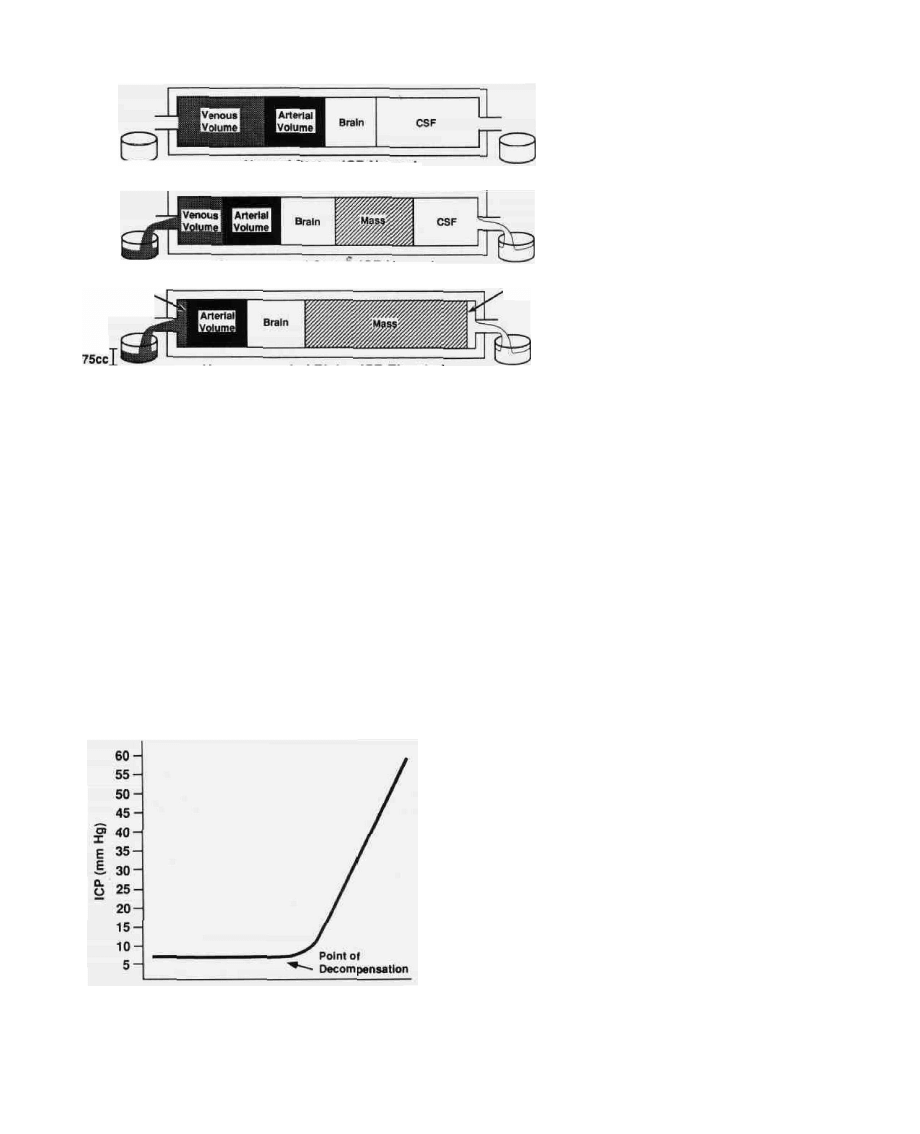
HEAD INJURY / 267
Normal State - ICP Normal
Venous
Volume
Compensated State"- ICP Normal
CSF
Uncompensated State - ICP Elevated
J.75CC
FIG. 16. The Monro-Kellie doctrine: intra-
cranial compensation for expanding
mass. The volume of the intracranial con-
tents remains constant. If the addition of
a mass such as a hematoma results in
the squeezing out of an equal volume of
CSF and venous blood, the ICP remains
normal. However, when this compensa-
tory mechanism is exhausted, there is an
exponential increase in ICP for even a
small additional increase in the volume of
the hematoma.
The Monro-Kellie Doctrine
This is a simple yet vitally important concept relating
to the understanding of ICP dynamics (152,153). It
states that the total volume of intracranial contents must
remain constant. This is fairly obvious because the cra-
nium is essentially a non-expansile box. Thus, if V de-
notes volume,
VBrain + Vcfs + F
Blood
+ F
Mass
= Constant
As the size of an intracranial mass lesion, such, as a
hematoma, increases, there is a compensatory squeezing
out of CSF and of venous blood (Fig. 16). The intracra-
nial pressure initially remains normal. However, eventu-
ally no more CSF or venous blood can be eliminated,
and the compensatory mechanisms are no longer effec-
tive. At this point, intracranial pressure begins to in-
crease exponentially with even a small additional in-
crease in the size of the intracranial mass. The
pressure-volume curve illustrates this phenomenon (Fig.
17). It is obvious from studying this curve that a normal
intracranial pressure does not necessarily preclude the
presence of a mass lesion. In fact, the ICP is generally
within normal limits until a patient reaches the point of
decompensation and enters the exponential phase of the
pressure-volume curve. The ICP number per se does not
initially give any indication of where along this curve a
patient is.
Brain Elastance
Volume of Mass
FIG. 17. Pressure-volume curve. The pressure-volume rela-
tionship described in Figure 1 6 is shown schematically in this
graph. Every effort should be made to keep the patient in the
flat portion of the curve rather than to try to salvage the pa-
tient once the point of decompensation has been reached.
In order to better understand ICP dynamics, the con-
cept of brain elastance was introduced. This is denned as
the change in ICP resulting from a unit change in intra-
cranial CSF volume. It is usually quantified in terms of
the "volume-pressure response" (VPR), which is defined
as the immediate rise in intracranial pressure resulting
from an injection of 1 ml of fluid over 1 second (154). In
a normal subject, the VPR is 0 to 2 mm Hg/ml. Values of
3 to 4 mm Hg/ml are often seen after surgery for head
trauma, and values of 10 to 20 mm Hg/ml are usually
indicative of the presence of a mass lesion.
Pressure- Volume Index
Another measure of intracranial compliance is re-
ferred to as the pressure-volume index (PVI). This is de-
nned as the volume of fluid that would theoretically have
to be injected into the craniospinal axis to produce a
10-fold increase in intracranial pressure (155). Clini-
268 CHAPTER 12
cally, this is a calculated figure based on the following
formula:
where P, is the initial ICP and P
2
is the final ICP after an
injection of, for example, 1 ml of fluid. Normal PVI is
26 ± 4 ml; values of 13 ml or less aft considered clearly
indicative of markedly compromised intracranial com-
pliance (156). Although VPR and PVI are not yet
widely used in the management of neurosurgical pa-
tients, it is important to understand their basis and sig-
nificance (157).
Cerebral Perfusion Pressure
Cerebral perfusion pressure (CPP) is the mean arterial
blood pressure minus intracranial pressure. Perfusion
pressures of less than 80 mm Hg are generally associated
with a poorer outcome following head injury (158). The
use of CPP rather than ICP alone has been recom-
mended by some for the routine monitoring of patients.
Rosner and Daughton have advocated a method of man-
agement of head injury based on maintenance of CPP
(159). Simard and Bellefleur have suggested that the po-
tentially deleterious effects of too great a perfusion pres-
sure following head injury may not have receiyed due
recognition (160).
Autoregulation
The phenomenon of autoregulation tends to maintain
a fairly constant cerebral blood flow (CBF) between
mean blood pressures of 50 and 160 mm Hg. Below 50
mm Hg the CBF declines steeply, and above 160 mm Hg
there is a passive dilatation of the cerebral vessels and an
increase in CBF. It has been shown that autoregulation is
often severely disturbed in the head-injured patient
(161). Because increases in cerebral blood volume can
contribute significantly to intracranial hypertension
(162), it is as important to avoid systemic arterial hyper-
tension as it is to avoid shock in the severely head-in-
jured patient. Although the data are not available regard-
ing the optimal level at which blood pressure should be
maintained, an overly aggressive correction of moderate
hypertension or less than prompt correction of hypoten-
sion can be disastrous, especially in elderly patients.
Technical Aspects
ICP Measurement in Different Planes
ICP can be monitored in several different planes
(163). These are given in the following list along with the
commonly available monitoring devices that can be
used:
• Lateral ventricle: ventricular catheter, pressure-sensi-
tive fiber-optic device
• Intraparenchymal: pressure-sensitive fiber-optic de-
vice
• Subdural/subarachnoid: hollow bolt, catheter, pres-
sure-sensitive fiber-optic device
• Epidural: pressure-sensitive capsule
• Anterior fontanel: tonometry
ICP Recording Devices
Three major types of devices are used for ICP moni-
toring. The intraventricular catheter remains the gold
standard. However, other devices are available and dem-
onstrate varying degrees of accuracy. The commonly
available devices include (1) catheters (intraventricular
or subdural); (2) hollow adapters (screws, bolts), such as
the Richmond, Philadelphia, Leeds, and Philips; and (3)
pressure-sensitive capsules such as the Camino fiber-op-
tic and Ladd devices.
We use ventricular catheters in almost all cases. For
the few instances in which the ventricles cannot be suc-
cessfully cannulated, we used to use subarachnoid (Rich-
mond) bolts, but over the last couple of years we have
been using the Camino fiber-optic device. Nevertheless,
the vast majority of our patients are still monitored
through a ventriculostomy. The advantages and disad-
vantages of these devices are shown in Table 10.
Value of ICP Monitoring
Although some debate persists regarding the indica-
tions for ICP monitoring in various neurosurgical condi-
tions, it is generally accepted that the technique can be
valuable in the monitoring and treatment of the severely
head-injured patient. ICP data can be used in three dif-
ferent ways:
1. As a diagnostic adjunct:
• Elevated ICP and midline shift on an air ventriculo-
gram serve as useful indicators of a mass lesion if a
CT scanner is not immediately available.
• ICP data facilitate early diagnosis of a developing
mass lesion.
• Data allow therapy to be initiated before irrevers-
ible neurological damage occurs, especially in se-
dated or paralyzed patients in whom the clinical
exam is difficult to follow.
2. As a therapeutic adjunct:
• Ventriculostomies are useful for CSF drainage,
which can lower ICP, at least temporarily.
• Knowledge of the ICP takes the guesswork out of
therapy. ICP fluctuates greatly, and the response of
different patients to different maneuvers to lower
ICP is very unpredictable. Empirical therapy with
HEAD INJURY / 269
TABLE 10. Features of certain ICP monitoring devices
agents such as mannitol, without a means of moni-
toring response, is therefore not optimal.
3. As a prognostic tool:
• In general terms, ICP trends can be used together
with clinical signs in judging prognosis.
Whether ICP monitoring per se improves outcome
from head injury is a rather controversial issue that has
been debated in neurosurgical conferences, as well as in
courts of law. Trying to prove this is somewhat akin to
trying to demonstrate that continuous blood pressure
monitoring improves outcome from cardiac surgery. In
view of the numerous variables involved, it is very diffi-
cult to design a study that would conclusively answer this
question. There has been no randomized study, and
such a study may be difficult to justify. However, certain
large, well-documented, nonrandomized studies have
indicated that as part of a program of intensive care, the
monitoring and control of ICP may be associated with
improved outcome in patients with severe head injury
(73,88,89). There is no doubt that ICP monitoring has
greatly added to our understanding of intracranial dy-
namics and helped put the management of patients on a
more scientific basis. We monitor ICP in all head injured
patients who have a significantly altered level of con-
sciousness and find the data so derived to be very valu-
able in patient management. However, facilities for ICP
monitoring are not universally available, and it is cer-
tainly feasible to use alternative management strategies
(164,165).
Indications for ICP Monitoring
Head injury is the most common indication for ICP
monitoring. As a general rule, patients who are able to
follow simple commands do not need to be monitored.
They may satisfactorily be followed clinically. In pa-
tients who are unable to follow commands and have an
abnormal CT scan, the incidence of intracranial hyper-
tension is high (53 to 63 percent) and monitoring is
warranted (30). Severely head-injured patients with nor-
mal CT scans generally have a low incidence of intracra-
nial hypertension (13 percent), unless they have two or
more of the following adverse features at admission (30):
1. Systolic blood pressure less than 90 mm Hg
2. Unilateral or bilateral motor posturing
3. Age over 40
ICP should be monitored in patients with cerebral
contusions who are unable to follow simple commands.
If the pressure rises and persists over 25 to 30 mm Hg,
surgical debridement is usually indicated. Clinicians
should be aware that ICP is not always elevated in the
presence of an intracranial process. This is particularly
true of temporal lobe lesions that can cause tentorial her-
niation in the absence of ICP elevation.
Treating Raised ICP
There has been some debate as to what constitutes
elevated ICP. Initially, it was decided somewhat arbi-
trarily to treat intracranial pressures of greater than 25
mm Hg in patients with severe head injury. Since then,
this figure has been moved down by other groups to 20
and then to 15 mm Hg. Transient elevations of ICP asso-
ciated with patient manipulation such as suctioning,
turning, or coughing do not constitute adequate reason
for treatment. The following step-wise approach to ICP
elevation is suggested:
Ventricular catheter
Subarachnoid bolt
Fiber-optic device
1 .
2.
1 .
2.
3.
1 .
2.
3.
.
Advantages
Gold standard of accuracy
Allows drainage of CSF for
• ICP control
• CSF sampling
• Monitoring infection
«
Does not invade brain
May have a lower infection rate
No need to cannulate ventricle
Can be placed subdurally,
intraparenchymally, or
intraventricularly
Minimal artifact and drift
High resolution of waveform
No need to reposition
transducer with change in
head position
1 .
2.
3.
4.
1 .
2.
1 .
2.
Disadvantages
Sometimes difficult to cannulate ventricle
Requires fluid-filled column, which can
get blocked by air bubbles and debris
Artifact from tube movement
Needs repositioning of transducer level
with change in head position
Blocking of port by swollen brain may
cause artificially low readings
Same as 3 and 4 under Ventricular
catheter
Inability to check calibration once
inserted, unless a ventriculostomy is
used simultaneously
Fiber breakage

270 CHAPTER 12
Ensure optimal body and neck position. It is generally
accepted that the neck should be in a neutral position
to facilitate venous drainage. Turning the neck to an
extreme position can result in reduced venous out-
flow and elevation of intracranial pressure. The opti-
mal degree of head elevation;remains somewhat con-
troversial. Though it has been generally believed that
raising the head of the bed was a uniformly useful
maneuver, certain authors argue that this has to
be individualized and that head elevation may in
fact adversely affect cerebral perfusion in certain
cases (159).
2. Check calibration. Before more involved steps are
taken to treat intracranial pressure, one must cali-
brate the monitoring system and make sure that the
readings are not artifactual.
3. Check serum Na
+
and ABGs. Hyponatremia is a
common problem in neurosurgical patients, often as
a result of SIADH. Hyponatremia should be treated
aggressively in these patients because it contributes
dramatically to brain swelling. Hypercarbia can also
result in brain swelling secondary to vasodilitation.
We used to use hyperventilation (down to a Pco
2
of
25 mm Hg) as a routine measure to treat patients with
potential brain swelling. Recent studies, however, in-
dicate that hyperventilation over a period of time
may contribute to cerebral ischemia owing to vaso-
constriction (H. F. Young, personal communication).
We therefore use this modality only when necessary,
and then for as short a time as needed to keep intracra-
nial pressure within normal limits.
4. Rule out seizures. Although they are not a common
occurrence, subclinical seizures may result in unex-
plained increases in intracranial pressure.
5. Rule out mass lesions with a CT scan. Elevated ICP is
a sign of problems and should not be considered a
diagnosis in and of itself. Hence, if the aforemen-
tioned measures do not resolve the ICP problem, a
CT scan of the brain should be obtained to make sure
there is no developing mass lesion. This cannot be
emphasized enough.
6. Hyperventilate to a Pco
2
of around 25 mm Hg. See
item 3 in this list.
7. Drain CSF via ventriculostomy. Intermittent drain-
age of CSF via the ventriculostomy is a very useful
method of controlling intracranial pressure. For this
reason a ventricular catheter is much more useful
than the other monitoring devices.
8. Administer mannitol (0.25 to 2.0 g/kg). This remains
our drug of choice for treating intracranial pressure
elevations. Although urea and glycerol have been
used in certain countries, mannitol is clearly the most
widely used agent in the United States. Its rapidity of
action, relative safety, and ability to be used intrave-
nously have contributed to its popularity.
9. Induce barbiturate coma. When all of the aforemen-
tioned measures have failed to control ICP, a barbitu-
rate coma may be considered. As a general guideline,
one should consider this when the ICP has remained
elevated over 25 mm Hg for 30 minutes or over 30
mm Hg for 15 minutes in spite of all of the preceding
therapies. The commonly used agent is pentobarbital
(Nembutal®) in a dose of 10 mg/kg as a loading dose,
over 30 minutes, 5 mg/Kg every 1 hour times 3, fol-
lowed by a maintenance dose of 1 mg/Kg/hr adjusted
to obtain a serum level of 3-4 mg% (142).
Complications of ICP Monitoring
The main risk of ICP monitoring is infection (30).
This incidence should be 5 percent or less. If monitoring
is conducted for less than three days, the infection rate is
virtually 0 percent. Beyond five days, the incidence of
infection begins to increase significantly. It is therefore
our practice to monitor for as short a duration as possi-
ble. If monitoring needs to be continued beyond five
days, the catheter is removed and a new catheter is in-
serted at a different site (166). The incidence of hemor-
rhage relating to the placement of an ICP monitoring
device is approximately 1 percent. The need for evacua-
tion of a catheter-related bleed is very uncommon. Fur-
thermore, because these devices are usually placed in the
frontal region, it is rare to have a neurological deficit
relating to catheter placement.
MANAGEMENT OF ASSOCIATED INJURIES
In a series of 100 patients admitted to the neurosurgi-
cal service of the Medical College of Virginia with severe
head injury, 57 had one or more major systemic injuries;
a total of 86 major injuries were recorded in these pa-
tients (10) (Table 4). Multiple injuries are most com-
monly associated with vehicular accidents (89 percent).
Falls and blows to the head account for only 11 percent
of the patients with multiple injuries. In view of the fre-
quency of other systemic injuries complicating the care
of the head-injured patient, a brief description of the
commonly encountered injuries and their management
is included.
Scalp Injuries
Scalp injuries are extremely common and are present,
to some degree, in almost all patients with a severe head
injury. The scalp consists of five layers (with the acro-
nym "SCALP"): skin, connective tissue (dense), apo-
neurosis (galea aponeurotica), loose connective tissue,
and pericranium. Its sensory nerve supply comes mainly
from the ophthalmic division of the trigeminal nerve an-
teriorly and the greater occipital nerve (C2) posteriorly.
Preauricularly, the auriculotemporal branch of the third

HEAD INJURY / 271
division of the trigeminal nerve follows the superficial
temporal artery, and the area behind the ear is supplied
by the lesser occipital nerve from the cervical plexus (C2
to C3). The scalp has a very rich blood supply from five
major arteries: the supratrochlear and supraorbital
branches of the ophthalmic artery anteriorly, and three
branches of the external carotid—superficial temporal,
posterior auricular, and occipital—laterally and posteri-
orly. These vessels lie in the second (dense connective
tissue) layer of the scalp. For this reason, the vessels do
not retract when cut and tend to bleed profusely. The
galea aponeurotica is a dense, fibrous, nonelastic layer
that attaches to the frontalis and occipitalis muscles. It is
vitally important to achieve good repair of this layer in
the closure of scalp wounds. The loose connective tissue
layer can collect large hematomas following blows and
houses the emissary veins that pass through the bone
into the dural sinuses. Bacteria and septic emboli can
travel from the scalp into the cranium by way of these
veins.
Although large scalp lacerations are hard to miss, the
same is not true for contusions and small lacerations in a
comatose patient. In fact, even gunshot wounds can be
missed in the absence of a leading history, only to be
found on more careful examination after skull x-rays
provide the physician with the correct diagnosis. Thus, it
behooves the physician to examine the scalp in an in-
jured patient.
Scalp lacerations should be thoroughly cleaned, ex-
plored, debrided, and closed. Perhaps the most common
errors made in the closure of such wounds are inade-
quate shaving of hair and inadequate cleaning of hair,
bone, and other debris from the wound. Although the
scalp is relatively forgiving because of its rich vascular
supply, a sloppy repair job in the emergency room can
result in needless and sometimes serious morbidity.
After shaving around the wound and irrigating it with
saline, the physician, using gloves, must explore the scalp
laceration and make sure there is no underlying fracture
or penetrating injury. If the bone feels normal, or if x-
rays confirm that only the outer table of the skull is in-
volved, the wound can be irrigated with Betadine solu-
tion and saline, the edges debrided with a scalpel, and the
wound closed with nonabsorbable sutures (3-0 nylon).
The timing of scalp repair is not crucial. If the patient is
harboring a mass lesion, the scalp can be repaired after
evacuation of the mass. If not, the repair can be accom-
plished in the emergency room or intensive care unit.
We prefer to use the operating room for more extensive
or complicated lacerations.
Scalp avulsions are less common but can be life-
threatening owing to the severe blood loss. The scalp is
usually avulsed through the loose connective tissue
layer. Direct microvascular anastomosis and replanta-
tion of the avulsed scalp is possible (167,168). For trans-
portation purposes, the avulsed scalp is cleaned with
normal saline, wrapped in damp sterile gauze, placed in
a watertight plastic bag, and transported on crushed ice.
There are many options for the design of skin flaps for
closure of scalp defects. In general, the larger the flap, the
poorer its chances of surviving. The base must be at least
as wide as or wider than the tip. Grafting procedures and
complex scalp reconstructions are generally performed
in conjunction with our plastic surgery colleagues. The
interested reader is referred to other sources for further
details (169-171).
Maxillofacial Injuries
A large proportion of patients admitted with multiple
trauma have evidence of maxillofacial injury (Table 11)
(172.173). In general terms, most facial injuries can be
handled semielectively several days after admission.
Even soft-tissue injuries can be repaired up to 24 hours
after admission in most cases. Exceptions to this rule
include acute airway obstruction secondary to retrodis-
placement of the tongue in bilateral mandibular fracture
and uncontrollable nasopharyngeal hemorrhage. How-
ever, despite the relatively low priority of definitive facial
injury treatment, emergency room evaluation—both
clinical and radiological—should not be side-stepped.
This will allow the plastic or oral surgeon to complete a
preliminary evaluation either before or during other
"emergency" operations and to choose whether to per-
form any stabilizing or reparative procedures while the
patient is under anesthesia. The general principles of
management of these injuries are summarized here, but
the interested reader is referred to an excellent chapter
on this subject by Manson (174).
The Water's view (occipitomental) is the most valu-
able x-ray for studying the maxilla, the zygoma, and the
frontal sinuses. Oblique views of the mandible give the
___TABLE 11. Classification of maxillofacial injuries
Soft-tissue injuries
A. Skin abrasions, punctures, lacerations, tattoos
B. Nerve injury—facial nerve branches
C. Parotid gland or Stensen's duct injury
D. Eyelid injury
E. Ear injury
F. Nasal injury
Bony injuries
A. Fractures of the upper third of the face
B. Fractures of the middle third of the face
1 . Nasal fractures
2. Maxillary fractures
LeFort I—transverse maxillary fracture
LeFort II—pyramidal fracture
LeFort III—craniofacial disjunction
3. Zygomatic fractures
4. Orbital fractures
C. Fractures of the lower third of the face
(mandibular fractures)
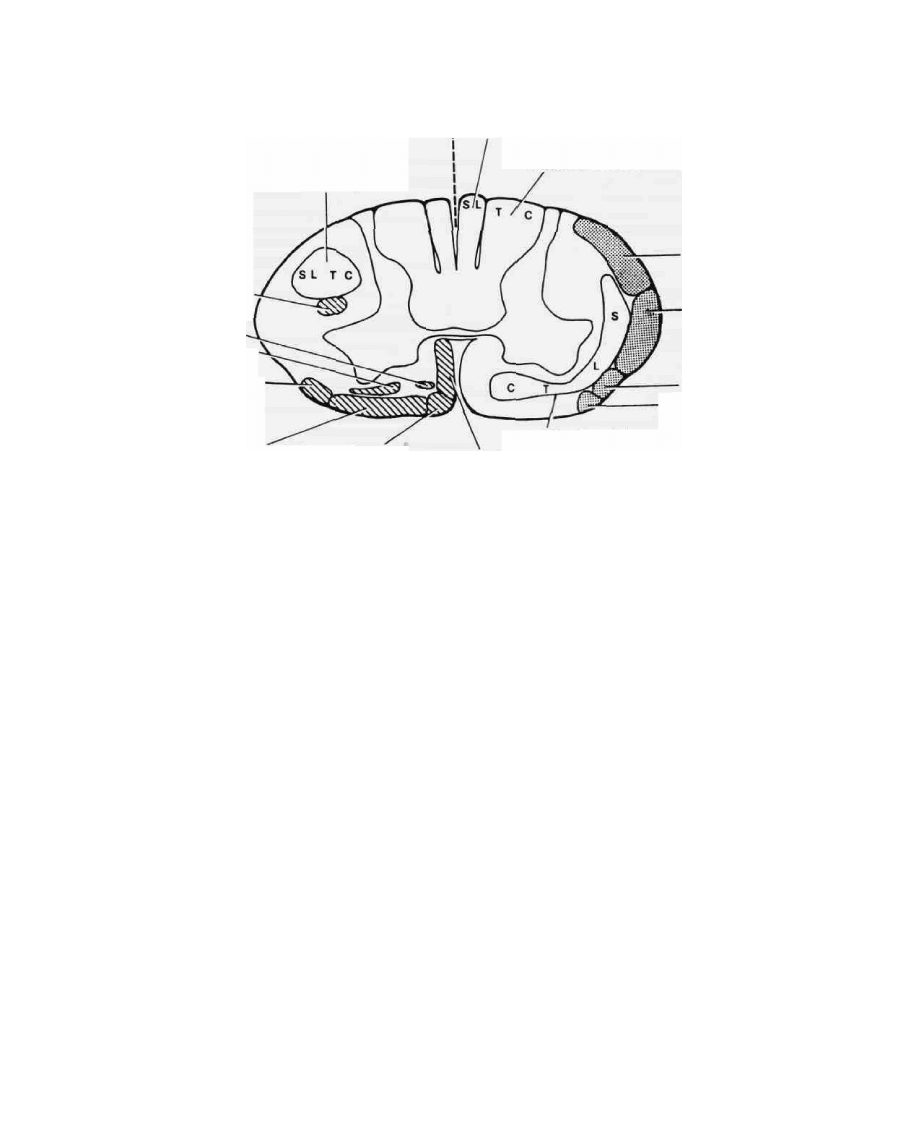
274 /
DESCENDING TRACTS
Lateral corticospinal
ASCENDING TRACTS
Fasciculus gracilis
Fasciculus cuneatus
Rubrospinal
Pontine
reticulospinal
Medullary
reticulospinal
Olivospinal
Dorsal
spinocerebellar
Ventral
spinocerebellar
Spino-olivary
Spinotectal
Vestibulospinal
Tectospinal
Ventral
corticospinal
Lateral & ventral
spinothalamic
FIG. 19. Cervical spinal cord. Cross section shows the tracts and the relative distribution of fibers.
C = cervical; T = thoracic; L - lumbar; S = sacral. (From reference 1 1 , with permission.)
of quadriparesis, usually worse in the distal upper extrem-
ities, and greater motor than sensory losses.
The final type of cervical spine injury is the accelera-
tion-deceleration, or whiplash, injury. Although it is not
life threatening, this type of injury has achieved great
medicolegal notoriety. A physical basis does, however,
exist—damage has been demonstrated in the anterior
supporting muscles, the longus colli, and also in the lat-
eral and posterior elements (189).
As stated earlier in the chapter, it behooves the physi-
cian to rule out the presence of a cervical spine injury in a
patient with head injury. In a conscious patient, nuchal
pain or tenderness may alert the physician to the pres-
ence of an injury. In a comatose patient, radiological
examination should be routinely performed before mov-
ing the patient. A lateral view, an anteroposterior view,
and an open-mouth view are usually initially adequate.
A swimmer's view may be necessary to visualize C6 to
C7 or C7 to Tl (Fig. 6). If there is any doubt, the neck
should be immobilized in a Philadelphia collar until a
definitive diagnosis can be made with polytomography
or a CT scan. High-resolution CT scanning has been
found to be clearly superior to plain films and polyto-
mography in the evaluation of spinal trauma and may
yield even more information in selected cases when
scans are obtained after a myelogram with water-soluble
contrast medium (190,191). If a significant fracture-sub-
luxation is detected and a CT scan rules out the need for
intracranial surgery, cervical traction is applied using
Gardner-Wells tongs or a halo ring without the jacket. If
reduction cannot be achieved with traction, open surgi-
cal reduction may be necessary at a later stage. Many
patients with unstable fractures can be successfully man-
aged with immobilization in a halo jacket for three
months, followed by the use of a Philadelphia collar for
several more weeks (192). However, there is a great deal
of variation in practice in this regard.
A distinction of significance in cervical spine injuries
is that between stable and unstable fractures (193). The
incidence of unstable fractures of the cervical spine is
around 25 to 30 percent (194,195). The following frac-
tures may be considered stable: compression or chip
fractures of the vertebral body, unilateral facet or lateral
mass fractures, and fractures of the spinous process. Dis-
location or subluxation indicates concomitant ligamen-
tous injury and implies instability. Stable fractures can
be managed with immobilization in a Philadelphia col-
lar. Sometimes instability that is not acutely apparent on
flexion-extension films as a consequence of splinting of
the spine by paraspinal muscle owing to pain may be-
come apparent on follow-up examination several days
later when the pain has subsided.
Some authors have recommended minimyelography
in the acute phase after spinal injury with neurological
deficits (196). The yield of this procedure is admittedly
low but may be undertaken if other more acutely life-
threatening problems have been dealt with. MRI is pre-
ferred whenever feasible.

HEAD INJURY / 275
Thoracic Spine
The thoracic spine is a relatively rigid and nonmobile
segment of the spine. This is reflected in the low inci-
dence of injuries to this area. However, when injuries do
occur, they indicate that large forces have been applied
and usually result in complete cord transection. Tho-
racic spine injuries are usually flexion injuries. Compres-
sion fractures may occur when axial forces are applied,
as when a person falls on the buttocks. These usually
occur at the thoracolumbar junction. The spinal cord
occupies a greater proportion of the canal in the thoracic
region than it does in the cervical or lumbar area. This
increases the likelihood of neurological injury when
bony damage occurs (197).
In the acute stage in patients with upper thoracic spine
injuries, one must consider the possibility of myocardial
contusion, aortic transecti'on or dissection, or lung inju-
ries. An aortogram may be necessary. It is important,
however, to stress basic immobilization and care during
patient transfer.
Most patients with thoracic spine fractures can be
managed with bed rest followed by an extension brace
for three to four months. However, surgical stabilization
may be preferable because it permits mobilization al-
most immediately. If there is clear-cut neurological dete-
rioration after admission, myelography or MRI should
be undertaken, and surgical intervention is required if
compression is found. Decompressive surgery may incor-
porate either Harrington or Luque rod stabilization or
may use a transthoracic approach (198,199). We have
recently been using pedicular screw fixation with Luque
plates for lower thoracic and lumbar fractures.
Lumbar Spine
Like the cervical spine, the lumbar spine is a mobile
segment and is therefore prone to injury, although less
frequently than the cervical spine. LI and L2 are the
most frequent sites for compression fractures. The conus
medullaris and cauda equina may be involved, resulting
in urinary incontinence and sexual dysfunction in the
male. The principles of management for these in-
juries are similar to those described for the thoracic
spine (200).
Orthopedic Injuries
Fractures can be classified simply as open (com-
pound) or closed. A closed fracture is one in which the
overlying tissues are intact, whereas in an open fracture
the bone is exposed and bacteria can directly enter the
fracture site. The initial treatment of fractures involves
splinting and, in some cases, traction. The agitated pa-
tient should have fractures splinted promptly to prevent
damage to contiguous nerves and major vessels in the
area of the fracture (201). The peripheral pulses distal to
a fracture must be checked periodically to make sure the
vessels are not being impinged upon. Peripheral neuro-
logic function is harder to assess in the comatose patient.
Large volumes of blood may collect in the area of a frac-
ture, and compartment syndromes may develop. These
require measurement of tissue pressures that, if clearly
elevated, call for fasciotomies for decompression. This
occurs more frequently in the upper extremity than in
the lower extremity.
Fat embolism is most frequently seen in patients with
long-bone fracture (202). Its etiology is not fully known.
Because the clinical syndrome is not pathognomonic
and the pathological findings are often scanty, the num-
ber of deaths attributable to this condition is unknown.
Some estimates place the figure as high as 16 percent of
all deaths related to trauma. In the fulminant form, the
previously awake and oriented patient becomes agitated,
rapidly lapses into lethargy and coma, and dies within a
few hours after injury. At autopsy, evidence of massive
fat embolism to the lungs, kidneys, brain, and other or-
gans is found. A definitive diagnosis antemortem is diffi-
cult because of the nonspecific nature of the refractory
shock syndrome. The classic form of fat embolization
appears somewhat later—24 to 72 hours postinjury—
and the symptoms are predominantly cerebral. The syn-
drome may initially present with sudden hypothermia,
followed by agitation, lethargy, stupor, and finally coma.
There is usually tachypnea, cyanosis, and pulmonary
edema as well. The presence of petechiae over the upper
portion of the body, conjunctiva, and in the fundi are
almost pathognomonic clinical signs. The finding of fat
in the urine or blood on microscopic exam is suggestive,
but a negative exam is meaningless. Arterial hypoxemia,
hypocarbia, and thrombocytopenia are common sys-
temic concomitants. Nevertheless, this often remains a
diagnosis of exclusion (203). The mortality rate is high
and is related to the depth and duration of coma. If the
patient does not die, there is usually a complete recovery.
Treatment is mainly supportive, with special attention
paid to ventilation.
Chest Injuries
Chest injuries are frequently encountered in the multi-
ply injured patient, and pulmonary complications fre-
quently affect the morbidity and sometimes the mortal-
ity associated with head trauma (204,205). Simple rib
fractures require no treatment other than analgesics and
possibly local infiltration with anesthetics to reduce pain
in a conscious patient. When several ribs are fractured,
however, a "flail chest" may result. In this condition, the
chest wall is no longer rigid, and paradoxic motion is
seen. This results in a loss of negative intrathoracic pres-

276 / CHAPTER 12
sure during inspiration, reduced ventilation, and possi-
bly atelectasis. It is believed that rather than the para-
doxic movement, the underlying pulmonary contusion
and wet lung may be the major source of respiratory
distress (206). For thisreason, fluid restriction to 1000 to
1200 ml/day, salt-poor albumin, and blood loss replace-
ment with colloids (whole blood, plasmanate) are sug-
gested. If the Po
2
and Pco
2
cannot be maintained within
satisfactory limits with these simple measures, as is the
case in 10 to 20 percent of patients, intubation and con-
tinuous positive-pressure ventilation (PEEP) are recom-
mended. Neurogenic pulmonary edema has been re-
viewed recently (207).
Aspiration pneumonitis is a frequent complication of
severe head injuries and should be avoided as carefully as
possible. It is advisable to place a Salem sump tube into
the stomach soon after intubation (with cuff inflated)
and to empty out the stomach. It is preferable and tech-
nically easier to pass the nasogastric tube prior to endo-
tracheal intubation, but an active gag reflex may initiate
a bout of vomiting during attempts to pass the tube; this
results in aspiration, with the physician having no con-
trol over the situation.
The indications for aortography in blunt thoracic
trauma have been reassessed by Gundry and associates,
who concluded that all trauma victims who have a wid-
ened mediastinum should undergo this procedure (208).
On reviewing their results in 173 patients who under-
went aortography to rule out traumatic rupture of the
thoracic aorta, they found mediastinal widening to be
the most reliable indication. According to the re-
searchers, "If you think the mediastinum looks widened,
you should obtain an aortogram." They did not find
other reported signs, such as obscuration of the aortic
knob or loss of sharpness of the aortic outline, to be valid
associations. However, in patients beyond puberty, any
evidence of a high-speed decelerating injury, including
pulmonary contusions and multiple rib fractures (espe-
cially ribs 1 and 2). was considered an adequate reason to
obtain an aortogram.
Cardiac Injuries
not universally, fatal. Large missile injuries or stab
wounds can result in rapid exsanguination, but small-ca-
liber injuries and even heart rupture from blunt trauma
can be successfully treated (210,211). Again, time is of
the essence. A patient with such an injury rapidly de-
velops signs of cardiac tamponade: distended neck veins,
plethoric appearance, hypotension (systolic pressure
falls more than diastolic pressure, resulting in a
narrowed pulse pressure), paradoxical pulse, muffled
heart sounds, and a widened mediastinum on percussion
and on chest x-ray.
Pericardial tamponade may be diagnosed by aspira-
tion with a 16- or 18-gauge needle inserted just to the left
of the xiphoid process at an angle 45° cephalad and 45°
to the right. Without moving the needle, as much blood
as possible is aspirated. Although this procedure can be
temporarily therapeutic, an open thoracotomy will prob-
ably be necessary if there is a significant cardiac defect
(201). Autotransfusion devices may be invaluable in the
management of these cases.
Cardiac Arrest
After trauma, the most common cause of cardiac
arrest is hypoxia and CO
2
retention secondary to inade-
quate ventilation. Perhaps of equal importance in the
trauma patient is hypotension caused by hypovolemia
and consequent coronary hypoperfusion. Other causes
include drug overdosage or hypersensitivity, and hyper-
kalemia or cardiac hypothermia owing to the rapid infu-
sion of cold banked blood. It should be stressed that most
of the precipitating causes for cardiac arrest in trauma
patients are preventable. A patient should be quickly in-
tubated and ventilated either at the scene of the accident
or on arrival to the emergency room, and hypovolemia
should be rapidly corrected. Drugs should be used with
care, especially in inebriated patients, who are particu-
larly sensitive to barbiturates and general anesthetics.
Once cardiac arrest has occurred, the team has about
three minutes to restore blood flow to the vital organs. If
the ventilatory and volume status has not been
corrected, this is the first priority.
Cardiac injuries may be either blunt or penetrating.
The former is usually due to the steering wheel impact-
ing on the anterior chest in an automobile accident. The
electrocardiogram may show ST-T changes, which
usually return to normal over a few days. There may be
an accompanying tachycardia. Although the prognosis
for a patient with cardiac contusion is generally good
(209,210), any surgery should be postponed if possible.
Cardiac isoenzymes may be followed to confirm the
diagnosis, although enzyme fractions may be elevated
secondary to associated injuries.
Penetrating injuries of the heart are often, although
Pneumothorax
Pneumothorax occurs frequently owing to laceration
of the lungs by fractured ribs, penetrating injuries, or
rupture of the tracheobronchial tree. It often leads to
collapse of the lung and decreased vital capacity. Clinical
signs of a pneumothorax include dyspnea, hyperreso-
nance on percussion, and absence of breath sounds over
the lung in question. A large pneumothorax can be de-
tected easily on a chest x-ray, but expiratory films of
good quality may be needed to define a smaller abnor-
mality. Though a patient can tolerate collapse of one

HEAD INJURY / 277
lung fairly well, air can get trapped in the pleural space
by a valve-like mechanism, resulting in a tension pneu-
mothorax. This causes shift of the mediastinum to the
opposite side, thus reducing the ventilatory capacity of
the "normal" lung as well. Unless corrected, this condi-
tion can prove fatal. Although a simple large bore needle
can serve as a temporary release valve, a chest tube must
be inserted as soon as possible.
A chest tube is inserted via a 1.5-cm incision in the
nipple line, where it transects the midaxillary line, using
a scalpel and a finger rather than a trocar. Two heavy silk
sutures are applied in a U-fashion to anchor the tube and
to close the hole later. The chest tube is connected to a
set of drainage bottles or a Pleurevac system, and a con-
tinuous negative pressure of 5 to 20 cm H
2
O is applied.
Trauma can result in a pure hemothorax, although a
hemopneumothorax is far more common. A hemotho-
rax of less than 300 ml is often not demonstrable on the
upright chest film. A large hemothorax usually presents
with shock secondary to the blood loss rather than respi-
ratory embarrassment. This condition is also corrected
with chest-tube drainage. Thoracotomy may be neces-
sary to overcome major vascular bleeding as from the
internal mammary, intercostals, or pulmonary vessels,
but this is uncommon.
Vascular Injuries
Peripheral vessels are sometimes damaged in the multi-
ple trauma patient, resulting in hemorrhage, arteriove-
nous fistulas, and aneurysms. Control of the hemorrhage
should be achieved immediately using compression.
Tourniquets often result in ischemic injury because they
are left on too long and collateral circulation is blocked
off as well. Ligation or prolonged clamping of the vessel
is also undesirable because it makes reconstruction more
difficult and endangers the survival of the limb.
All injuries in the area of a major blood vessel should
be assumed to involve the vessel, unless proven other-
wise (212). The presence of a distal pulse does not ex-
clude the presence of a vascular injury. Arteriograms
should be performed in such cases, although even these
studies can sometimes be misleading.
Blunt injury to the neck may produce severe extra-
cranial carotid artery spasms or intimal dissection. This
may, in turn, result in a stroke, thus confounding an
already complex picture secondary to the head injury.
Abdominal Injuries
Abdominal injuries, like chest injuries, are either pen-
etrating or blunt. The former are more acutely lethal, but
the latter are more difficult to diagnose and can be the
source of considerable delayed morbidity. Unexplained
shock, in association with abdominal trauma, is due to
abdominal injury unless proven otherwise. Indications
for prompt laparotomy are evidence of peritonitis, unex-
plained shock, gastrointestinal bleeding, and a positive
diagnostic abdominal tap or lavage. An abdominal tap is
first performed (213). If over 20 ml of blood is obtained
or if food particles or feces are evident in the peritoneal
cavity, the tap is considered positive. If not, one liter of
lactated Ringer's or normal saline is infused into the ab-
domen. The patient is then rolled from side to side to
allow good mixing, and the fluid is allowed to flow back
out. When 200 to 300 ml of fluid has been removed, it is
sent for a stat cell count. A count of over 100,000 red
blood cells or 500 white blood cells per cubic mm is
considered positive. Butterworth and associates have
made a strong case for routine peritoneal lavages in pa-
tients with severe head injury "whether or not clinical
signs of shock, abdominal injury, or occult hemorrhage
are present" (38). Peritoneal lavages arc also of value in
detecting hemorrhage in patients with spinal cord inju-
ries, in whom the usual clinical signs may be masked
(214,215). Recent studies indicate that abdominal CT
scanning may be superior to peritoneal lavages in the
evaluation of blunt abdominal trauma (216,217). How-
ever, these studies can take over half an hour to com-
plete, thus limiting their usefulness in patients with intra-
cranial masses or marked instability (217,218).
Renal Injuries
Kidney injuries consist of three main types: (1) renal
contusion; (2) renal laceration, with or without urinary
extravasation; and (3) pedicle injury. Hematuria is the
primary finding in injuries of the urinary tract. It is often
gross but may be microscopic or absent. Abdominal pain
is usually present in the conscious patient. Examination
may reveal evidence of shock, local tenderness, swelling,
and ecchymosis. There is usually marked muscle spasm
in the flank and upper quadrant of the abdomen.
An intravenous pyelogram followed by nephroto-
mography, if necessary, must be obtained whenever kid-
ney injury is suspected. This will not only provide evi-
dence of distortions of the renal or ureteral systems but
also confirm the presence and proper functioning of the
contralateral kidney. CT scan of the abdomen is the test
of choice if the anatomy is not well delineated by these
tests, and aortography may be indicated in select cases.
Most renal injuries (85 percent) are contusions and can
be managed conservatively. The other 15 percent are
major lacerations. Most of these (95 percent) are well
contained and can also be managed nonsurgically. In
about 5 percent of cases, however, surgical intervention
is necessary (219,220). Pedicle injuries also call for ur-
gent exploration. Ureteral injuries are uncommon com-
plications of trauma, being iatrogenic far more often.
Drainage of urine and reconstruction of the ureter is the

278 CHAPTER 12
treatment of choice. Upper urinary tract extravasation is
generally associated with a better outlook than lower uri-
nary tract extravasation because the latter is often asso-
ciated with injuries of the bladder and bowel.
Ophthalmological Injuries
When an eye injury is noted at the site of the accident,
it is best to cover it with a rigid shield such as a Foxx
shield. Manipulation of the eye, so as to remove a blood
clot or foreign body, should be avoided because a simple
wound can be converted into one with extensively her-
niated ocular contents (221). Detailed examination can
be deferred until an ophthalmologist sees the patient in
the hospital emergency room.
Patients who have been involved in an automobile
accident often have foreign bodies in their eyes, usually
glass from the windshield or debris from the roadside. In
a conscious patient, such foreign bodies would cause se-
vere discomfort and alert the physician to the problem.
In an unconscious patient, however, they can be over-
looked and lead to further damage. If a foreign body is
suspected, the eye should be thoroughly irrigated with
normal saline using a syringe. If a foreign body is embed-
ded in the cornea or conjunctiva and does not flush out,
mechanical removal may be necessary. This can be ac-
complished with an applicator moistened with saline,
but such a maneuver can result in the loss of consider-
able corneal epithelium. Ideally, the body should be re-
moved with the aid of a slit lamp or corneal microscope
and a fine hypodermic needle. Local antibiotics such as
gentamycin may be prescribed. Because of the danger of
infection, the patient should be seen by an ophthalmolo-
gist each day, and the cornea should be stained with fluo-
rescein until healing has occurred. In any case, fluores-
cein staining should be performed on admission
whenever a superficial eye injury is suspected in order to
rule out a corneal/conjunctival abrasion, which could
become infected if ignored.
The presence of intraocular foreign bodies is usually
not suspected, so they are commonly overlooked. This
possibility must be excluded whenever an eye appears to
have a large or small laceration or penetrating injury. If
even a small foreign body remains in the eye, it may
cause blindness from hemorrhage, infection, or retinal
detachment. The location of a foreign body may be de-
termined using ophthalmoscopy, slit-lamp examination,
dental film, CT scans, ultrasonography, or a combina-
tion of these. Generally, all foreign bodies should be re-
moved, with a few exceptions. The eye may tolerate inert
material such as lead, glass, aluminum, and certain types
of plastic. Organic matter such as wood or plant mate-
rial, however, usually causes an overwhelming inflamma-
tory reaction. In any case, systemic antibiotic coverage is
used until danger of infection is passed. Sympathetic
ophthalmia, which is thought to be an autoimmune
uveitis, can result in loss of the uninjured eye, but it is
exceedingly uncommon. Any doubtful eye should be
carefully observed for at least a year, although 80 percent
of cases present in the first three months postinjury.
Once the disease is established, adrenocorticotropic hor-
mone (ACTH) and steroid therapy can be helpful, but
the results are usually dismal.
In certain cases of corneal laceration, atropine or pilo-
carpine may be useful to retract the iris from the wound.
However, these agents should be avoided in patients
with severe head injury, at least in the initial period. This
is especially important when the patient is intubated and
paralyzed and the only means of detecting impending
herniation syndrome is by checking pupillary size and
reactivity. Once a diagnosis has been established and the
patient is in a stable condition with ICP monitoring in
place, these agents may be used. Pupillary dilatation per-
mits a more detailed examination of the fundus and may
also be therapeutic in an inflamed eye.
Most often the ocular fundus is normal, even with
severe head injury. Small or large intraretinal hemor-
rhages are sometimes seen, but they are of little conse-
quence to the overall neurological condition. Although
swollen optic discs are occasionally reported to occur
within minutes of raised intracranial pressure, papille-
dema is seen in a minority of patients with serious head
injuries. Moreover, swelling of the optic discs is usually
not seen until the third to fifth day, sometimes after de-
compression of an intracranial mass and relief of ele-
vated intracranial pressure. This delay is curious, be-
cause the papilledema is attributed to axonal dilation as
a result of mechanical impediment to axoplasmic flow.
Severely attenuated retinal arteries are occasionally due
to very high intraocular pressure from massive swelling
of traumatized orbital tissue. Retinal and optic nerve
infarction follow. This situation is potentially reversible,
if recognized early, by a simple lateral canthotomy.
Various types of traumatic retinopathies have been re-
ported (222). One type is Purtscher's retinopathy, which
consists of multiple scattered hemorrhages in the super-
ficial layers of the retina and deep white areas in the
posterior poles. This injury is associated with sudden ele-
vations in systemic venous pressure, as occurs with crush
injuries or forceful impacts on the chest or abdomen.
SEQUELAE OF HEAD INJURY
CNS injury is a dynamic process. It is generally ac-
cepted that the more severe the impact suffered, the
worse the ultimate outcome is likely to be. Perhaps less
well recognized is the fact that soon after the initial in-
jury, a wide variety of secondary processes come into
play. These sequelae can have a major impact on the
patient's eventual level of recovery. It is not uncommon

HEAD INJURY 279
to see two patients with similar initial injuries have
widely disparate outcomes, at least partly as a result of
complications. Whereas certain secondary insults occur
in the acute phase, other complications arise or are no-
ticed in the subsequent weeks and months. This section
summarizes the current thinkingaon some of the more
commonly encountered long-term sequelae of head in-
jury.
Cranial Nerve Injuries
Cranial Nerve I
The incidence of olfactory dysfunction after head
trauma has been reported as varying from 2 to 38 per-
cent. Damage to the olfactory system occurs with great
frequency in occipital blows, but the incidence is even
higher after frontal injury. It is the most commonly in-
volved cranial nerve after minor head injury. Impaired
olfactory recognition may result from focal and diffuse
injury to the orbitofrontal and temporal regions. Animal
studies have implicated a role for olfaction in the tem-
poral lobe. Anosmia will occur in almost 50 percent of
patients who sustain rhinorrhea from an anterior fossa
fracture and in about 50 percent of those who require
surgical repair. Spontaneous recovery of functional ol-
faction may occur in more than one-third of patients
over a period of days to five years after injury (223).
Cranial Nerve II
Injury to the visual system occurs in 5 percent of all
patients who sustain head trauma, regardless of severity.
Traumatic loss of vision may occur without overt evi-
dence of injury to the eye. It typically results from an
ipsilateral blow, usually frontal, occasionally temporal,
and rarely occipital. It may occur after minor head in-
jury.
Direct pupillary response to light is the most reliable
early indicator of the extent of optic nerve injury. Oph-
thalmoscopic examination and x-rays are studies of sub-
stantially less value. Unilateral eye injury can be identi-
fied by the presence of decreased to absent pupillary
reactivity to light stimulation, with preservation of the
consensual reaction (Marcus-Gunn pupil). The unin-
volved eye maintains a normal light reflex but impaired
consensual response. These reactions indicate an affer-
ent lesion—usually in the optic nerve—in the pupillary
light reflex pathways.
Visual-evoked potentials may provide valuable objec-
tive information even during coma, because patient co-
operation is not essential. This procedure is more accu-
rate than clinical examination in the early diagnosis of
retrobulbar visual dysfunction. CT scans are particularly
valuable in assessing the integrity of the optic canal.
As coma resolves, the patient should be evaluated for
light perception. Serial evaluations should be under-
taken for the presence of visual fixation as well as for
localization and tracking of stimuli. The optokinetic re-
sponse may provide evidence of preservation of an
acuity level of 20/200 in at least part of the visual field.
The term "cortical blindness" should be reserved for
patients who demonstrate amaurosis with reactive pu-
pils, not for individuals who have incurred partial visual
field loss. Most patients with cortical blindness will re-
gain some limited visual capability via secondary visual
pathway systems. The patient's response to high-inten-
sity moving stimuli should be evaluated. The patient
who is cortically blind with denial of the visual loss (An-
ton's syndrome) has usually suffered bilateral occipital
lobe infarctions secondary to posterior cerebral artery
compression at the tentorial edge caused by herniation.
Cranial Nerves HI, IV, and VI
Extraocular muscle dysfunction causes diplopia and
may result from central or peripheral motor dysfunc-
tion. Diplopia may contribute to the confusion of the
patient arousing from coma. Eye patching can abolish
the double image, but when the patient has the ability to
suppress the second image, eye patching should be dis-
continued. The common practice of alternating the
patch between the affected and the unaffected eye is
meant to prevent amblyopia. However, because amblyo-
pia does not occur in the adult population, it is reason-
able to patch the sound eye to stimulate maximal motor
activity of the affected eye.
Abnormal head postures may be utilized to compen-
sate for paretic extraocular motor function. This com-
monly occurs in cranial nerve IV paresis. The fourth
cranial nerve is not only a depressor but also an intorter
of the eye; the patient tends to compensate by tilting the
head. Attempts at normalizing the head position may
prevent the patient from achieving binocular vision.
Head tilt may also result from nystagmus, because stabi-
lizing the head against the shoulder may dampen the
nystagmus. Visual field deficits also frequently produce
head turning in order to align the remaining visual field
properly.
Spontaneous resolution of paresis of eye movements
occurs with considerable frequency. In cranial nerve III
paresis, a residual superior rectus weakness may remain,
and the patient may complain of occasional diplopia.
Cranial nerve IV lesions spontaneously resolve in 65 per-
cent of unilateral involvement and in 25 percent of the
bilateral cases (224). Though some have argued that sur-
gical correction in permanent paralysis may be merely
cosmetic, Fells and Waddell have demonstrated that res-
toration of binocularity can occur in the majority of
cases (225).

280 / CHAPTER 12
Cranial Nerve V
Injury of the trigeminal nerve is relatively uncommon.
The patient who demonstrates an insensitive cornea, as
indicated by an absent corneal reflex, in the presence of
facial nerve paresis (especially if the lacrimal branch is
involved) is at great risk to develop repeated neurotro-
phic corneal ulceration and possible loss of vision. These
patients should be considered early for protective tar-
sorrhaphy. Protective lubricants should be used liberally
as part of routine nursing. Tear production, regulated by
the lacrimal branch of the facial nerve, may be evaluated
by the Schirmer tear test.
Cranial Nerve VII
The status of the facial nerve must be documented at
the initial examination. If paralysis is of immediate on-
set, and CT demonstrates compromise of the facial
canal, prompt exploration for nerve decompression may
be undertaken. The facial nerve traverses a longer bony
canal than does any other cranial nerve and is therefore
extremely vulnerable to injury. Ten to 30 percent of lon-
gitudinal fractures of the temporal bone and 30 to 50
percent of transverse fractures result in facial nerve
palsy.
If there is delayed development of paralysis, the prog-
nosis is substantially better if the paralysis is not bilat-
eral, and the patient should be followed with serial facial
nerve testing. Neurophysiologic testing including nerve
conduction and electromyographic studies should dem-
onstrate some signs of recovery within eight weeks, if
recovery is to occur. In such cases exploration is proba-
bly not necessary, because complete recovery occurs in
75 percent of the cases and partial recovery in 15 per-
cent.
Cranial Nerve VIII
The inner ear is the most commonly damaged sensory
organ after severe head injury. Vertigo may occur as a
result of vestibular apparatus damage or labyrinthine
concussion. Hearing loss is primarily conductive as a re-
sult of ossicular chain disruption or blood in the middle
ear. The ossicular chain is most often disrupted at the
incudostapedial joint. Surgical intervention and pros-
thetic replacement of the dislocated component are es-
sential for restoration of hearing.
Transverse fractures of the petrous portion of the tem-
poral bone usually produce sensorineural hearing loss.
The labyrinthine capsule is generally disrupted, resulting
in severe vestibular and cochlear damage, including
functional destruction of the semicircular canals, utricle,
and saccule. Because the fracture line in transverse frac-
tures is perpendicular to the facial nerve, both nerves are
damaged in 50 percent of patients with this fracture.
Assessment of oculovestibular responses may provide
early information regarding the status of the system, and
later electronystagmography may confirm end-organ
impairment of the vestibular nerve. No reliable diagnos-
tic test of central vestibular nerve function is available.
Brainstem auditory-evoked potentials can contribute sig-
nificantly to the evaluation of the integrity of auditory
nerve and cochlear nucleus, but they provide little in-
sight into the structure or function of the vestibular
nerve component.
Locked-in Syndrome
The terms "locked-in syndrome" and "akinetic mut-
ism" are used synonymously. Damage to the corticobul-
bar and corticospinal pathways in the ventral pons re-
sults in a de-efferented state characterized by tetraplegia
and mutism. The patient remains aware and responsive,
and higher cortical function remains unaffected.
Supranuclear ocular pathways are spared so that eye
movement control is at least partially preserved, usually
in the vertical and sometimes in the horizontal plane.
Nonoral communication is therefore possible, either uti-
lizing eye movements or blinking, and the use of appro-
priate interface systems can provide sufficient communi-
cation with which to demonstrate retained cognitive
abilities. The syndrome results most often from vascular
infarction and, therefore, is not commonly found as a
result of trauma. Locked-in syndrome must be clearly
differentiated from the vegetative state in which sen-
tience is not preserved, despite a return of sleep-wake
cycles and a deceptive appearance of neurologic recov-
ery ("coma vigil") that frequently gives the patient's fam-
ily and friends an unjustified sense of optimism.
Peripheral Neuropathies
Polyneuropathies are reported as an early complica-
tion of sepsis and other critical illnesses in up to 50 per-
cent of patients in intensive care units (226). This com-
plication is occasionally recognized clinically in
head-injured patients. The neuropathy usually subsides
as the critical illness comes under control. Neuropathies
associated with fractures can occur at the fracture site.
However, compression neuropathies can result from im-
mobility and localized pressure to a nerve over a bony
prominence. Such compression most commonly affects
the ulnar and peroneal nerves. Whenever a limb remains
flaccid, the possibility of neuropathy exists. In the uncon-
scious patient, physical evaluation can be quite limited,
and nerve-conduction studies may be valuable.
Plexopathies involve many muscle groups, so that
tone is diminished from what would be expected. Direct
injury to the shoulder or the pelvis may result in stretch-
ing, contusion, compression, or laceration injuries to the
brachial or lumbosacral plexuses. The pattern of flacci-

dity in an extremity should alert one to reevaluate the
force mechanisms of the initial injury and to consider
appropriate electrophysiologic studies. If bone fracture
has occurred, excessive callift development may result in
adjacent nerve compression, with late development of
nerve injury.
Posttraumatic Hydrocephalus
Definition
The syndrome of posttraumatic hydrocephalus (PTH)
must be denned using both radiologic and neurologic
criteria, because both features must be present to make
the diagnosis. In simple terms, PTH may be described as
ventricular dilation without sulcal enlargement, asso-
ciated with a clinical syndrome that may vary from deep
coma to the typical picture of normal-pressure hydro-
cephalus: dementia, ataxia, and urinary incontinence
(see also Chapter 9, "Hydrocephalus").
Incidence
Although ventricular dilatation is a common finding
after head injury, particularly when the injury is severe,
true PTH is relatively uncommon. The incidence of
posttraumatic ventricular dilatation has been variously
reported to be between 29 and 72 percent (227). Obvi-
ously, differences in diagnostic methods, definition of
ventricular enlargement, and patient characteristics
must account for these wide differences. Kishore and
coworkers defined significant ventriculomegaly as a dis-
tended appearance of the anterior horn of lateral ventri-
cles, enlargement of the temporal horns and third ventri-
cle, and normal or absent sulci (228). They then
prospectively followed 100 consecutive severely head-in-
jured patients with serial CT scans of the head for over a
year. Twenty-nine patients developed ventriculomegaly
within the year, and 27 of the 29 developed it within the
first two weeks.
Cardoso and Galbraith reported a retrospective review
of possibly a more heterogenous group of 2374 patients
with severe head injury (229). Of this group of patients
(who were not scanned or followed according to a prede-
termined protocol), 17 (0.7 percent) developed symp-
tomatic hydrocephalus. Of these, eight patients (47 per-
cent) improved markedly, and four (24 percent) slightly,
after shunting.
In a CT study performed at least three months after
head injury, Gardeur and associates found ventricular
enlargement in 78 percent of the patients (230). Simi-
larly, van Dongen and Braakman reported CT evidence
of cerebral atrophy in 86 percent of patients examined
one to four years after closed head injury resulting in
coma for at least six hours (231). Levin and coworkers
studied the area of the lateral ventricles on CT scans
HEAD INJURY / 281
obtained at least 30 days after severe closed head injury
in 32 young adults and reported enlargement in 72 per-
cent of the cases (232).
Posttraumatic hydrocephalus must be distinguished
from posttraumatic cerebral atrophy. The former term
denotes an active, treatable condition, which com-
pounds existing neurologic deficits, whereas the latter
represents brain parenchymal resorption secondary to
diffuse tissue injury. Unfortunately, this distinction is
not always readily apparent. CT scanning has certainly
made the diagnosis easier to make, and. interestingly,
there has been a drop in the reported incidence of PTH
to between 1 and 8 percent, as compared with 21 to 36
percent in the pneumoencephalogram era (233,234).
Pathophysiology
It is generally believed that PTH results from an im-
pairment in the flow and absorption of CSF. Although
radiologic and pathologic evidence suggests that this
blockage is usually around the cerebral convexities, it is
certainly possible that blockage of the arachnoid granu-
lations by subarachnoid blood may play a role (235). In
any case, subarachnoid hemorrhage seems to be a fea-
ture common to these two hypotheses.
Clinical Features
PTH may be manifested in a variety of ways. As re-
ported by Kishore and colleagues. 27 of the 29 patients
in their series developed the syndrome within two weeks
of injury (228). There is a reported case of ventricular
enlargement within seven hours of a head injury, result-
ing in a rapidly deteriorating level of consciousness and
early herniation. However, more delayed presentations
are certainly possible. In fact, remote trauma is rather
commonly reported in series of patients with normal-
pressure hydrocephalus (NPH).
PTH may present as classic NPH, with dementia,
ataxia, and urinary incontinence. However, altered lev-
els of consciousness and even coma may occur as part of
the syndrome. Because severe head injury often results
in fairly extensive neurologic dysfunction, these features
may be hard to separate from the effects of brain trauma
in the acute phase. Intracranial pressure monitoring and
serial CT scans can be useful in this setting. In the more
chronic phase of recovery, a deteriorating level of con-
sciousness, decreasing functional capacity, or any of the
features of NPH should serve as a tip-off. Some atypical
manifestations, such as emotional problems, bilateral
extensor responses, seizures, and leg spasticity, have also
been reported.
Radiologic Features
Kishore and coworkers have used the following CT
criteria to define hydrocephalus: (1) distended appear-

282 / CHAPTER 12
ance of the frontal horns of the lateral ventricles; (2) en-
largement of the temporal horns and the third ventricle;
(3) normal or absent sulci; and (4), if present, enlarge-
ment of the basal cisterns and fourth ventricle. Periven-
tricular lucency was used as an indicator of communicat-
ing hydrocephalus. Ex vacuo ventriculomegaly, or
atrophy, is characterized by diffuse ventricular enlarge-
ment with prominent sulci and no periventricular lu-
cency. Levin and colleagues used ventricular area as cal-
culated from a CT scan to study the relationship between
ventriculomegaly and neuropsychologic deficits after
closed head injury (232). Although this technique is
clearly the most accurate way of assessing ventricular
size, there is no radiologic method that can reliably pre-
dict outcome following shunting.
Periventricular edema has been recognized as a patho-
logic and radiologic feature of hydrocephalus. Normally,
fluid from the brain parenchyma moves across the epen-
dymal lining into the ventricles. In the presence of hydro-
cephalus, this normal direction of flow is reversed, and
fluid moves from the ventricles into the periventricular
white matter. Since T
2
-weighted MRI images are very
sensitive for water, it was hoped that this technique
would define the population with symptomatic hydro-
cephalus. Unfortunately, this is not quite so simple.
Zimmerman and associates reported that a review of 365
consecutive MRI studies revealed some degree of peri-
ventricular hyperintensity (PVH) in 93.5 percent of
cases, regardless of diagnosis (236). Of the six patients in
their series with NPH, two had mild nonspecific PVH
and four had prominent PVH, but in all cases multiple
white matter hyperintense foci (presumably representing
infarctions) were also present. The degree of PVH was
similar to that seen in nonhydrocephalic elderly pa-
tients and could therefore not be used as a criterion for
shunting.
Selection of Patients for Shunting
There is no single clinical, radiologic, or physiologic
feature that can serve as an accurate and infallible crite-
rion for shunt placement. Needless to say, if there is se-
vere underlying brain damage, shunting, even if it is in-
dicated, may not improve functional outcome
significantly. Nevertheless, every patient should be care-
fully evaluated and given the benefit of the doubt, be-
cause shunting can make a difference in a substantial
number of cases. Approximately 50 percent of patients
with ventriculomegaly will improve significantly after
shunting. If a patient meets the clinical and radiologic
criteria defined earlier, every effort must be made to ob-
tain an assessment of the craniospinal axis pressure. If
the patient has an ICP monitor in place, this information
is readily available. If not, a lumbar puncture can be
performed with the patient lying flat on his or her side,
and the ICP recorded when he or she is relaxed and the
abdomen is not being compressed. No firm pressure
guidelines are available in PTH for shunting. It stands to
reason that if the lumbar CSF pressure is lower than 136
mm H
2
O (10 mm Hg), a shunt is unlikely to help, but if
it is higher than 276 mm H
2
O (20 mm Hg), it may be
very useful. However, when the pressures are in between,
this single reading does not provide a clear answer.
Draining 20 to 30 ml of CSF may sometimes result in
significant, albeit transient, clinical improvement, thus
tipping the balance in favor of shunting.
When the lumbar pressure is normal, shunting may be
considered if a classic picture of NPH exists. Salmon
found that five of nine posttraumatic patients with this
syndrome improved after shunting regardless of other
test results (237). If the picture is not clear, a brief period
(12 to 48 hours) of ICP monitoring may be helpful. In
one study of 12 subjects, patients who showed variable
ICP improved following shunt surgery, but those with
consistently flat ICP tracings did not (238). Brgesen,
Gjerris, and Srensen, however, reported that ICP data
per se did not help them in a series of patients with
"true" NPH who had mean ICPs not exceeding 12 mm
Hg (239). In this series, they reported that conductance
to CSF outflow was a much more relevant measurement,
but this method has not become widely used in clinical
practice.
Cisternography has been extensively used in the past
in the evaluation of patients with NPH. When a radionu-
cleotide is injected into the lumbar subarachnoid space,
it normally flows over the cerebral convexities and is
absorbed into the major venous sinuses via the arach-
noidal granulations. When the normal flow of CSF over
the convexities is impeded, the isotope backs into the
ventricles within an hour of the injection and lingers
there for 24 to 72 hours. Although this ventricular reflux
was thought to be typical of NPH, its correlation with
improvement after shunting has been only fair. Cister-
nography plus an assessment of the clinical picture, com-
bined with lumbar or intracranial pressure monitoring
and neuropsychological testing, form the basis for selec-
tion for shunting.
Cerebrospinal Fluid Fistulas
Definition
A traumatic cerebrospinal fluid fistula may be defined
as a CSF leak occurring as a consequence of a head in-
jury. Fistulas may present as rhinorrhea, otorrhea, or
pneumocephalus.
Incidence
CSF fistulas reportedly occur in 0.25 to 3.0 percent of
all patients with a head injury and in 5 to 11 percent of
HEAD INJURY / 283
those with a basal skull fracture (240-242). An estimated
150,000 cases of traumatic rhinorrhea occur in the
United States each year (243). In one series, CSF oto-
rrhea occurred in 7 percent of 300 basal skull fractures
(244). In this same series, pneumocephalus occurred in
about one-third of patients with rhinorrhea, although
this may be an isolated finding (244).
CSF Rhinorrhea
This condition occurs in about 25 percent of patients
with an anterior basal fracture. CSF may leak via the
frontal sinus (through the cribriform plate or orbital
plate of the frontal bone), via the sphenoid sinus, and.
less frequently, via the clivus. On occasion, with a frac-
ture of the petrous part of the temporal bone. CSF may
enter the eustachian tube and, if the tympanic mem-
brane is intact, drain from the nose. Drainage begins
within 48 hours of injury in almost 80 percent of cases
(245,246). The fluid is watery and nonmucoid, and it
contains glucose. A glucose concentration of 30 mg/100
ml or greater is very suggestive of CSF. Dextrostix and
similar products are unreliable because normal nasal se-
cretions may give a positive reaction, but protein electro-
phoresis combined with immunofixation for an isoform
of transferrin has recently been shown to be useful in
identifying CSF (247).
Several aspects of the management of CSF rhinorrhea
remain controversial, including the use of prophylactic
antibiotics, the timing of surgery, and the role of lumbar
drains. In general, 80 percent of fistulas will stop leaking
within one week (248). The patient should be nursed in a
position that stops or minimizes the leak. If the leak has
not stopped in about three days, a lumbar subarachnoid
drain should be inserted and allowed to drain at about
shoulder level for three to seven days. If the leak persists
at 10 to 14 days, surgery should be considered, and diag-
nostic testing should be initiated to identify the site of the
leak. lohexol (Omnipaque) CT cisternography is
currently considered to be the diagnostic test of choice
(249). In an intermittent CSF leak, however, this test
may give a false negative result. Various maneuvers,
such as the Trendelenberg position, Valsalva's maneu-
ver, and lumbar subarachnoid saline injection, have
been described to maximize the probability of detecting
the site of leakage (250).
Once the fistula site has been identified, it can be sur-
gically repaired using an intracranial (intradural or ex-
tradural) or a transsphenoidal approach, depending on
the site of the leak. Sense of smell may be lost as a result
of the initial injury, especially with fractures of the eth-
moidal bone. The incidence of anosmia may be as high
as 80 percent. An intracranial frontal fossa floor repair is
associated with a high incidence of anosmia, even when
smell is normal preoperatively. The extradural repair
technique may be advantageous in this regard (251). The
size of the defect may be rather small, and the surgeon
may face some difficulty in finding the dural tear. Lyoph-
ilized dura, pericranium, or fascia lata is often used to
patch the defect. We have used human fibrin adhesive to
provide an additional seal.
CSF Otorrhea
This condition occurs when the petrous bone is frac-
tured, the overlying dura mater and arachnoid are torn,
and the tympanic membrane is perforated. Fractures of
the petrous bone are classified as longitudinal or trans-
verse, based on their relationship to the long axis of the
petrous pyramid; however, most fractures are mixed. Pa-
tients with a longitudinal fracture present with conduc-
tive hearing loss, otorrhea, and bleeding from the exter-
nal ear. Patients with a transverse fracture generally have
a normal tympanic membrane and demonstrate sensori-
neural hearing loss from damage to the labyrinth, coch-
lea, or the eighth nerve within the auditory canal. Facial
paresis is present in up to 50 percent of patients (252).
Longitudinal fractures are four to six times more fre-
quent than transverse fractures, but they are much less
likely to cause facial nerve injury-.
CSF otorrhea ceases spontaneously in the overwhelm-
ing majority of patients within a week. The incidence of
meningitis in patients with otorrhea is probably about 4
percent, as compared with 17 percent with CSF rhinor-
rhea. In the rare event that it does not cease, lumbar
drainage and even surgery may be undertaken.
Prophylactic Antibiotics
The role of prophylactic antibiotics in the manage-
ment of CSF otorrhea or rhinorrhea remains uncertain
because of a paucity of data, and their use is therefore
varied in different centers. The only prospective random-
ized study of the use of penicillin in patients with rhin-
orrhea or otorrhea was limited to 52 patients (253). Men-
ingitis developed in only one patient in study, and this
occurred in a placebo-treated patient who had an intra-
ventricular foreign body. The authors concluded that
their study did not support the routine use of prophylac-
tic antibiotics in these cases.
Posttraumatic Vascular Complications
Definition
Posttraumatic vascular complications can involve
both the arterial and the venous systems and may occur
either extracranially or intracranially. They are usually
noted at the time of initial impact, or soon after the in-

284 CHAPTER 12
jurv is sustained, but occasionally may not become ap-
parent until several days or even months after the injury.
Incidence
The true incidence of vascular complications asso-
ciated with head injury is unknown because of the lim-
ited number of epidemiologic studies. Furthermore,
with cerebral angiography having been virtually elimi-
nated from the routine evaluation of head-injured pa-
tients since the advent of CT, this database is not likely to
be improved upon. It is important, therefore, that clini-
cians maintain a high index of suspicion and obtain an-
giograms when the clinical picture cannot be explained
by the CT or MRI scans. One study of 2000 head-injured
civilians reported a 4.2-percent incidence of vascular in-
juries (254).
Classification
Posttraumatic vascular complications may be classi-
fied as follows:
A. Arterial
1. Cervical
a. Direct carotid or vertebral artery transection
b. Thromboembolic occlusion from a traumatic
nidus or intimal dissection
c. Traumatic arterial aneurysms
d. Traumatic arteriovenous fistulas
2. Intracranial
a. Thromboembolic occlusion
b. Traumatic aneurysms
c. Traumatic arteriovenous fistulas
d. Carotid-cavernous fistulas
B. Venous
1. Dural venous sinus thrombosis
C. Traumatic vasospasm
Discussion
The interested reader is referred to an excellent review
by Kassell, Boarini, and Adams (255). Penetrating inju-
ries of the neck obviously call for angiography and surgi-
cal exploration if the platysma has been penetrated. Arte-
rial occlusion secondary to blunt neck trauma occurs
infrequently, with an estimated incidence of 0.5 percent.
The injury- is said to occur most commonly at the C2
leveL with both the carotid and vertebral arteries. Clini-
cal diagnosis is often difficult, and there may be a symp-
tom-free period, usually of less than 24 hours. The pa-
tient may experience transient ischemic attacks, form a
neck hernatorna, or develop Horner's syndrome. Once
occlusion occurs, a focal neurologic deficit may become
apparent. In cases of severe head injury, this may be hard
to separate from the effects of the primary brain injury.
The mortality rate for traumatic carotid thrombosis in
the neck is reportedly between 40 and 90 percent. Verte-
bral artery occlusions are less frequently documented
and have a lower associated mortality: 19 percent when
one vertebral artery is occluded and 46 percent when
both are occluded. Anticoagulation medications may be
given in selected patients in whom the head injury is
mild and the risk of intracranial hemorrhage is low; how-
ever, the value of anticoagulation treatment in these pa-
tients has not been established.
Posttraumatic intracranial aneurysms are very un-
common. A study by El Gindi and associates reported
only seven cases among 2000 head-injured patients
(254). Furthermore, there were only two such aneurysms
in more than 3000 penetrating head wounds reported
from the Korean and Vietnam wars. Unlike congenital
"berry" aneurysms, posttraumatic aneurysms are more
likely to occur near the cortical surface than at major
arterial bifurcations. There is often no neck for clipping,
but surgical exposure and clipping or wrapping remains
the treatment of choice.
Intracranial traumatic arteriovenous fistulas are also
uncommon. They occur most often between the middle
meningeal artery and a meningeal vein. They are usually
associated with a penetrating head injury or a depressed
skull fracture. The risk of hemorrhage from these lesions
is uncertain. They can be treated by embolization via the
external carotid artery or by direct surgical excision.
Carotid-cavernous (CC) fistulas are the best recog-
nized of all posttraumatic vascular injuries. Although rel-
atively uncommon, their characteristic features make
them a well-recognized clinical entity. Sixty to 80 per-
cent of CC fistulas are traumatic in origin; the rest pre-
sumably arise spontaneously. Spontaneous CC fistulas
occur more commonly in older women, whereas those
from trauma are found more commonly in young men.
The clinical features can include proptosis, chemosis,
bruit, ophthalmoplegia, visual deterioration, and head-
ache. A bruit may be palpable, and a murmur can be
heard with a conventional or Doppler stethoscope. Arte-
riography is the diagnostic procedure of choice. The natu-
ral history of CC fistulas warrants intervention: spontane-
ous closure is uncommon, and the usual course is one of
progressive visual loss (40 to 50 percent will develop
blindness), intolerable bruit, or disfiguring proptosis (see
also Chapter 4, "Aneurysms and Carotid-Cavernous Fis-
tufas"). Although various approaches have been used for
their treatment, the current treatment of choice is occlu-
sion of the fistula with a detachable balloon, with preser-
vation of blood flow in the carotid artery (256). When
this is not technically possible, various alternative ap-
proaches may be used, including balloon occlusion of
the internal carotid artery, packing of the posterior cav-
ernous sinus with thrombogenic material or wire, and
occlusion of the sinus by packing via the ophthalmic
vein.
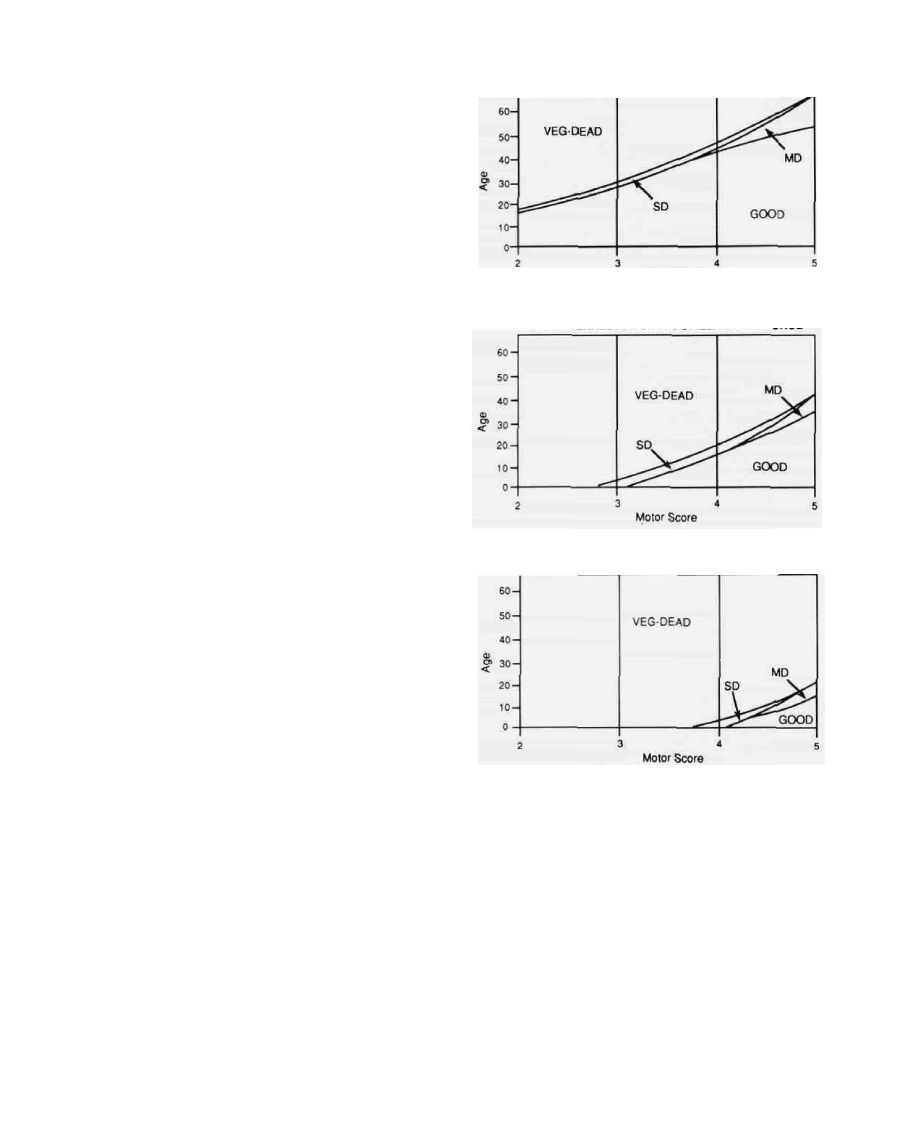
PROGNOSIS
The Glasgow Outcome Scale (GOS) has been widely
accepted as a standard means of describing outcome
in head injury patients. This is a simple five-point
scale (257):
Good recovery [G]
Moderately disabled
[MD]
Severely disabled
[SD]
Vegetative [V]
Dead [D]
Patient returns to preinjury
level of function
Patient has neurological
deficits but is able to look
after self
Patient is unable to look after
self
No evidence of higher mental
function
These categories can be lumped together as either good
outcome (G, MD) or poor outcome (SD, V, or D). Based
on logistic regression, a method has been described for
assigning patients into one of these two categories. This
method has been described in detail elsewhere (258). A
simpler method is based on discriminate analysis and
can assign patients into one of four outcome categories
(G, MD, SD, or V/D) (259). Only age, pupillary re-
sponse, and motor score are required for this. (Fig. 20).
This model was based on data collected from 523 pa-
tients with a severe head injury. If a prediction fell into
the correct outcome group, this was termed specifically
accurate. If an outcome group adjacent to the actual out-
come was accepted, the prediction was described as
grossly accurate. With this model, the overall specific
prediction rate was 78 percent and the grossly accurate
prediction rate was 90.4 percent. It should be pointed
out that the polar predictions—good recovery and death
—are much easier to predict accurately than the inter-
mediate categories of moderately or severely disabled. It
should also be noted that these prediction models are
based on neurological function alone, whereas mortality
can often result from unexpected medical complica-
tions. The value of such predictions lies in the clinician's
ability to counsel the patient's family and possibly to
compare the effect of newer therapies on smaller groups
of patients, with statistically predicted outcomes based
on past experience.
Unfortunately, the resources available for medical
treatment are often finite, and difficult decisions some-
times must be made regarding the optimal allocation of
efforts. A recent analysis by Gibson and Stephenson
showed that mortality after severe head injury could be
predicted with 100 percent accuracy in about 15 percent
of patients who reached their intensive care unit (260).
This simple bedside scale may be useful in identifying
that subgroup of patients in whom a fatal outcome is
virtually assured regardless of maximal therapeutic ag-
gfessiveness.
HEAD INJURY / 285
BILATERALLY NORMAL PUPILLARY RESPONSE
Motor Score
UNILATERALLY ABSENT PUPILLARY RESPONSE
BILATERALLY ABSENT PUPILLARY RESPONSE
FIG. 20. Predicting outcome in severe head injury. Outcome
can be predicted at admission with a reasonable degree of
accuracy based on three clinical indicators: pupillary re-
sponse, age, and motor response. (From reference 259, with
permission.)
CONCLUSION
Head injury is a common and potentially devastating
disorder with vast socioeconomic implications. The out-
come from head injury is influenced by various factors,
including the severity of the initial impact, associated
injuries suffered, and the occurrence of secondary com-
plications—both systemic and cerebral.
Major advances have been made over the past two
decades in the classification of this disease and explora-
tion of its pathophysiology. Significant reduction in mor-
tality and morbidity associated with severe head injury
has been achieved with aggressive management proto-

286 / CHAPTER 12
cols that emphasize early ventilatory control, minimal
delay to surgical evacuation of mass lesions, careful con-
trol of intracranial pressure, maintenance of adequate
cerebral perfusion, and optimization of the intracranial
milieu. The anatomic basis of mild and moderate head
injury is beginning to be better understood. Current ef-
forts in the field are being directed at the development
and clinical testing of new drugs and physiological inter-
ventions. It is anticipated that further improvements in
the field will be derived from the cumulative benefit of
several such interventions. Historically, advances made
in the field of neurotrauma have generally had a favor-
able impact on a variety of other neurological disorders.
ACKNOWLEDGMENTS
The author wishes to express his sincere gratitude to
Stephanie Goldfield for preparing this manuscript, Me-
linda Mosheim for organizing and preparing the photo-
graphs, Sangita Rangala for researching the references,
Jan Redden for the excellent illustrations, and Dr. Win-
ifred Hamilton for helping to pull it all together. Parts of
this chapter are derived from chapters I wrote for D. P.
Becker and S. K. Gudeman (262) and M. Rosenthal
(263) and are used with the permission of the publishers.
REFERENCES
1. U.S. Department of Health, Education and Welfare. Facts of life
and death. Publication HRS 74-1222, 1974.
2. Kraus JF. Epidemiology of head injury. In: Cooper PR, ed. Head
Injury, 2nd ed. Baltimore: Williams and Wilkins, 1987;1-19.
3. Gissane W. The nature and causation of road injuries. Lancet
1973;2:695-698.
4. Trunkey DD. Trauma. Sci Am 1983;249:28-35.
5. Centers for Disease Control. Morbiditv and mortality weekly re-
port 1982;31:599.
6. Centers for Disease Control. Morbidity and mortality weekly re-
port. 1988:37:1-68.
7. The Commission on Trauma Research, The Commission on Life
Sciences, The National Research Council, and The Institute of
Medicine. Injury in America: a continuing public health problem.
Washington, DC: National Academy Press, 1985;!.
8. Kraus JF, Black MA, Hessol N, et al. The incidence of acute brain
injury and serious impairment in a denned population. Am J
Epidemiol 1984;! 19:186-201.
9. Kalsbeek WD, McLaurin RL, Harris BS 3rd, Miller JD. The Na-
tional Head and Spinal Cord Injury Survey: major findings. J
Neurosurg 1980;53(Suppl 5):19-31.
10. Miller JD, Sweet RC, Narayan RK, Becker DP. Early insults to
the injured brain. JAMA 1978;240:439-442.
11. Narayan, RK. Emergency room management of the head-injured
patient. In: Becker DP, Gudeman SK, eds. Textbook of head in-
jury. Philadelphia: WB Saunders, 1989;23-66.
12. Teasdale G, Jennett B. Assessment of coma and impaired con-
sciousness. Lancet 1974;2:81-84.
13. Jennett B, Teasdale G. Assessment of impaired consciousness. In:
Jennett B, Teasdale G, eds. Management of head injuries. Phila-
delphia: FA Davis, 1981;77-93.
14. Miller JD. Minor, moderate and severe head injury. Neurosurg
Rev 1986:9:135-139.
15. Williams DH, Levin HS, Eisenberg HM. Mild head injury classifi-
cation. Neurosurgery 1990;27:422-428.
16. Jennett B. Teasdale G. Early assessment of the head injured pa-
tient. In: Jennett B, Teasdale G, eds. Management of head inju-
ries, 3rd ed. Philadelphia: FA Davis, 1981;99.
17. Seelig JM, Becker DP, Miller JD, Greenberg RP, Ward JD, Choi
SC. Traumatic acute subdural hematoma: major mortality re-
duction in comatose patients treated within four hours. N Engl J
Afe/1981;304:1511-1518.
18. Gennarelli TA. Cerebral concussion and diffuse brain injuries. In:
Cooper PR, ed. Head injury, 2nd ed. Baltimore: Williams & Wil-
kins, 1987;108-124.
19. Maull KI. Alcohol abuse: its implications in trauma care. South
MedJ 1982;75:794-798.
20. Rimel RW, Giordani B, Barth JT, Jane JA. Moderate head in-
jury: completing the clinical spectrum of brain trauma. Neurosur-
gen- 1982:11:344-351.
21. Dacey RG Jr, Alves WM, Rimel RW, Winn HR, Jane JA. Neuro-
surgical complications after apparently minor head injury: assess-
ment of risk in a series of 610 patients. J Neurosurg 1986;65:203-
210.
22. Fowkes FGR, Ennis WP, Evans RC, Roberts CJ, Williams LA.
Admission guidelines for head injuries: variance with clinical
practice in accident and emergency units in the UK. Br J Surg
1986:73:891-893.
23. Masters SJ. McClean PM, Arcarese JS, et al. Skull x-ray examina-
tions after head trauma: recommendations by a multidisciplinary
panel and validation study. N Engl J Med 1987;316:84-91.
24. Bruno LA. Gennarelli TA, Torq JS. Management guidelines for
head injuries in athletics. Clin Sports Med 1987;6:17-29.
25. Wilberger JE. Marvon JC. Head injuries in athletes. Clin Spans
Med 1989:8:1-9.
26. Rockswold GL. Leonard PR, Nagib MG. Analysis of manage-
ment in thirty-three closed head injury patients who "talked and
deteriorated." Neurosurgery 1987;21:51-55.
27. Hoff JT. Anderson TE, Cole TM, eds. Mild to moderate head
injun: Boston: Blackwell, 1989.
28. Stone JL, Lowe RJ. Jonasson O, et al. Acute subdural hematoma:
direct admission to a trauma center yields improved results. J
Trauma 1986:26:445-450.
29. Milter JD. Butterworth JF, Gudeman SK, et al. Further experi-
ence in the management of severe head injury. J Neurosurg
1981:54:289-299.
30. Narayan RK, Kishore PR, Becker DP, et al. Intracranial pressure:
to monitor or not to monitor? A review of our experience with
severe head injury. J Neurosurg 1982;56:650-659.
31. Levine JE. Becker D, Chun T. Reversal of incipient brain death
from head-injury apnea at the scene of accidents. N EnglJ Med
1979:301:109 [letter].
32. Weigelt JA. Initial management of the trauma patient. Crit Care
Clin 1986:2:705-716.
33. Zachariades N, Rapidis AD, Papademetriou J, Koundouris J, Pa-
pavassiliou D. The significance of tracheostomy in the manage-
ment of fractures of the facial skeleton. J Maxillofac Surg
1983:11:180-186.
34. Gordon L, Ponten LI. The nonoperative treatment of severe head
injuries. In: Vinken PJ, Bryun GW, eds. Handbook of clinical
neurology, vol 24. Amsterdam: Elsevier, 1976;599-626.
35. Chestnut RM, Marshall LF. Analysis of the role of secondary
brain injury in determining outcome from severe head injury.
American Association of Neurological Surgeons' annual meet-
ing, Nashville, 1990.
36. Parsa MH, Tabora F. Central venous access in critically ill pa-
tients in the emergency department. Emerg Med Clin North Am
1986;4:709-743.
37. Simpson ET, Aitchinson JM. Percutaneous infraclavicular sub-
clavian vein catheterization in shocked patients: a prospective
study in 172 patients. J Trauma 1982;22:781-784.
38. Butterworth JF 4th, Maull KI, Miller JD, Becker DP. Detection
of occult abdominal trauma in patients with severe head injuries.
Lancet 1980;2:759-762.
39. Borovich B, Braun J, Yosefovich T, Guilburd JN, Grushkiewicz
J, Peyser E. Intracranial penetration of nasogastric tube. Neuro-
surgery 1981;8:245-247.
40. Wyler AR, Reynolds AF. An intracranial complication of naso-
gastric intubation. J Neurosurg 1977;47:297-298.
41. Maloney AF, Whatmore WJ. Clinical and pathological observa-
tions in fatal head injuries: a 5-year survey of 173 cases. BrJSurg
1969;56:23-31.
Wyszukiwarka
Podobne podstrony:
ZX50 cap 12 (plastiche)
ZX50 cap 12 (plastiche)
wykład 12 pamięć
Figures for chapter 12
Mechanika techniczna(12)
Socjologia wyklad 12 Organizacja i zarzadzanie
CALC1 L 11 12 Differenial Equations
zaaw wyk ad5a 11 12
budzet ue 11 12
zapotrzebowanie ustroju na skladniki odzywcze 12 01 2009 kurs dla pielegniarek (2)
Stomatologia czesc wykl 12
Etyka 12
RI 12 2010 wspolczesne koncepcje
więcej podobnych podstron