
Chronic Kidney Failure
Przemyslaw Rutkowski MD, PhD

Objectives
•Kidney Failure
•Stages of Chronic Kidney Disease
•Definition and Classification of CKD
• Etiology
• Proteinuria
• GFR

Definition of CRF
Structural or functional abnormalities of the
kidneys for >3 months, as manifested by
either:
1. Kidney damage, with decreased GFR, as defined by
• pathologic abnormalities
• markers of kidney damage, including abnormalities in the
composition of the blood or urine or abnormalities in
imaging tests
2. GFR <60 ml/min/1.73 m
2
, with kidney damage

Definition of ESRD vs Kidney Failure
• ESRD is a federal government defined
term that indicates chronic treatment by
dialysis or transplantation
• Kidney Failure: GFR < 15 ml/min/1.73
m
2
or on dialysis.

Classification of CRF by Diagnosis
• Diabetic Kidney Disease 19,8%
• Glomerular diseases
(autoimmune diseases,
systemic infections, drugs, neoplasia) 23,75%
• Vascular diseases
(renal artery disease,
hypertension, microangiopathy) 12%
• Tubulointerstitial diseases
(urinary tract infection,
stones, obstruction, drug toxicity) 15%
• Cystic diseases
(polycystic kidney disease) 9%
• Diseases in the transplant
(Allograft nephropathy,
drug toxicity, recurrent diseases, transplant
glomerulopathy)
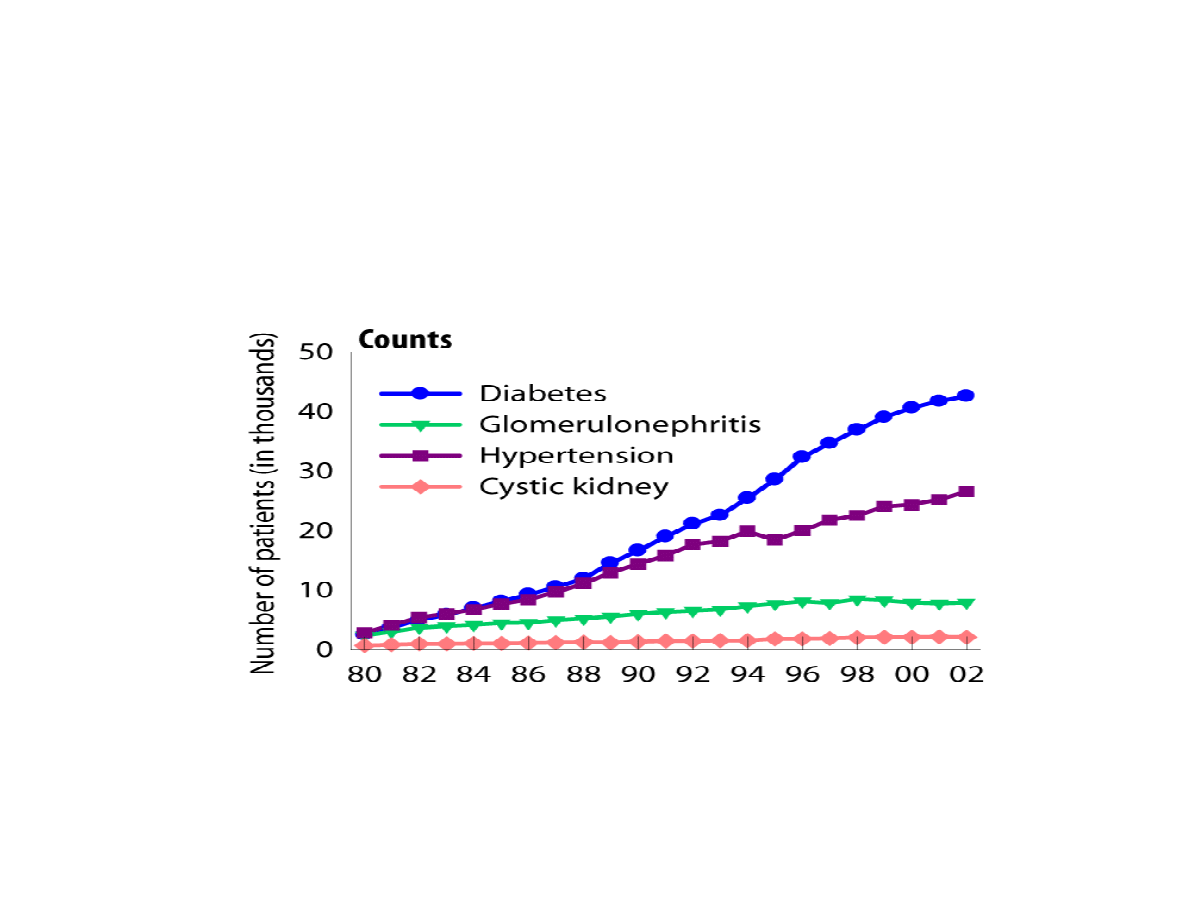
Incident Counts & Adjusted Rates,
By Primary Diagnosis
USRDS, 2004
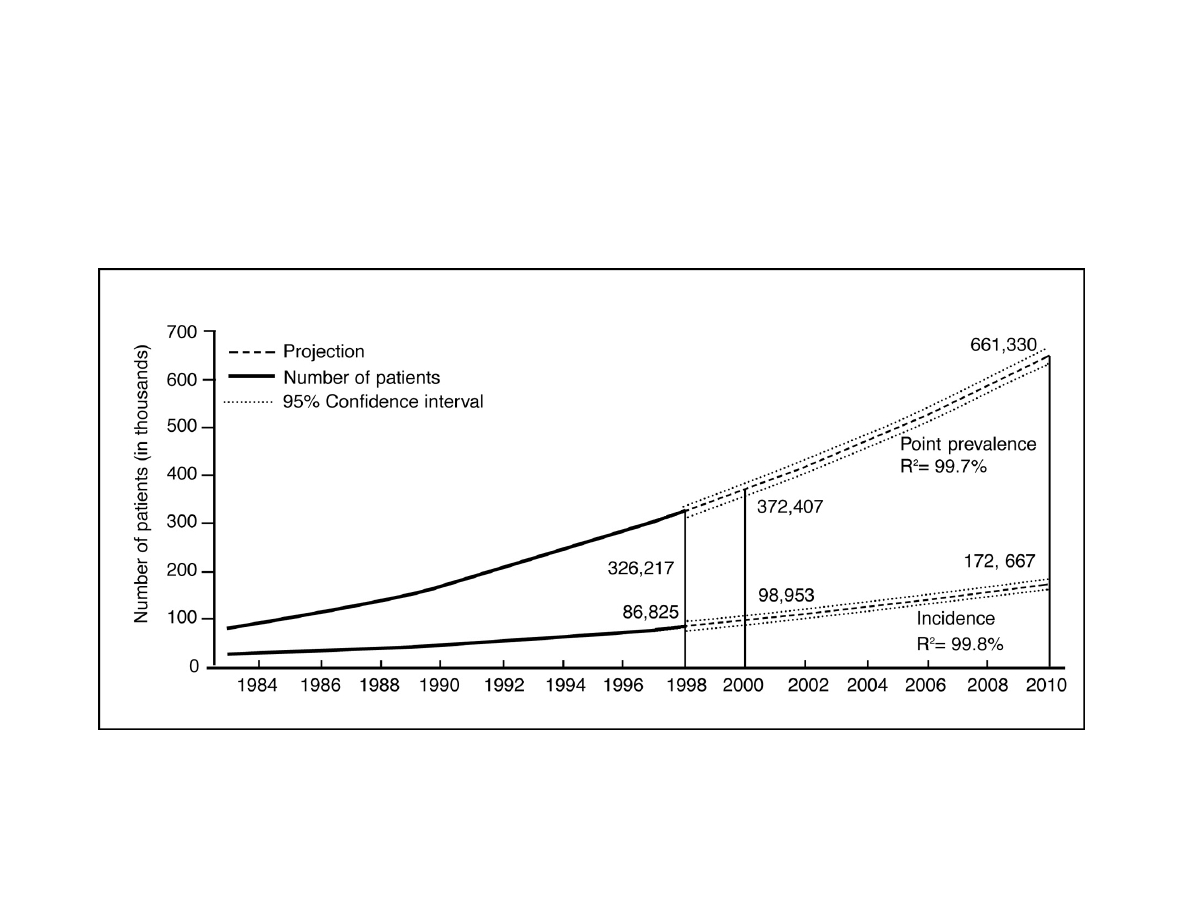
Incidence and Prevalence of End-Stage
Renal Disease in the US
Cardiovascular Mortality in the General
Population and in ESRD Treated by Dialysis
0.01
100
10
1
0.1
Annual mortality (%)
25–34
45–54
65–74
≥
≥
≥
≥85
35–44
55–64
75–84
Male
Female
Black
White
Dialysis
General population
Age (years)
CKD
death
CKD
CKD
death
death
Stages in Progression of Chronic Kidney
Disease and Therapeutic Strategies
Complications
Complications
Complications
Screening
Screening
for CKD
for CKD
risk factors
risk factors
CKD risk
CKD risk
reduction;
reduction;
Screening for
Screening for
CKD
CKD
Diagnosis
Diagnosis
& treatment;
& treatment;
Treat
Treat
comorbid
comorbid
conditions;
conditions;
Slow
Slow
progression
progression
Estimate
Estimate
progression;
progression;
Treat
Treat
complications;
complications;
Prepare for
Prepare for
replacement
replacement
Replacement
Replacement
by dialysis
by dialysis
& transplant
& transplant
Normal
Normal
Normal
Increased
risk
Increased
Increased
risk
risk
Kidney
failure
Kidney
Kidney
failure
failure
Damage
Damage
Damage
↓
↓
↓
↓ GFR
↓
↓
↓
↓
↓
↓
↓
↓
GFR
GFR

Prevalence of CKD and Estimated Number
of Adults with CKD in the US
(NHANES 88-94)
%
N
(1000s)
0.1
300
< 15 or Dialysis
Kidney Failure
5
0.2
400
15-29
Severe ↓ GFR
4
4.3
7,600
30-59
Moderate ↓ GFR
3
3.0
5,300
60-89
Kidney Damage with
Mild ↓ GFR
2
3.3
5,900
≥ 90
Kidney Damage with
Normal or ↑ GFR
1
Prevalence*
GFR
(ml/min/1.73 m
2
)
Description
Stage
*Stages 1-4 from NHANES III (1988-1994). Population of 177 million with age ≥20. Stage 5 from USRDS (1998), includes
approximately 230,000 patients treated by dialysis, and assuming 70,000 additional patients not on dialysis. GFR estimated
from serum creatinine using MDRD Study equation based on age, gender, race and calibration for serum creatinine. For
Stage 1 and 2, kidney damage estimated by spot albumin-to-creatinine ratio ≥17 mg/g in men or ≥25 mg/g in women in two
measurements.
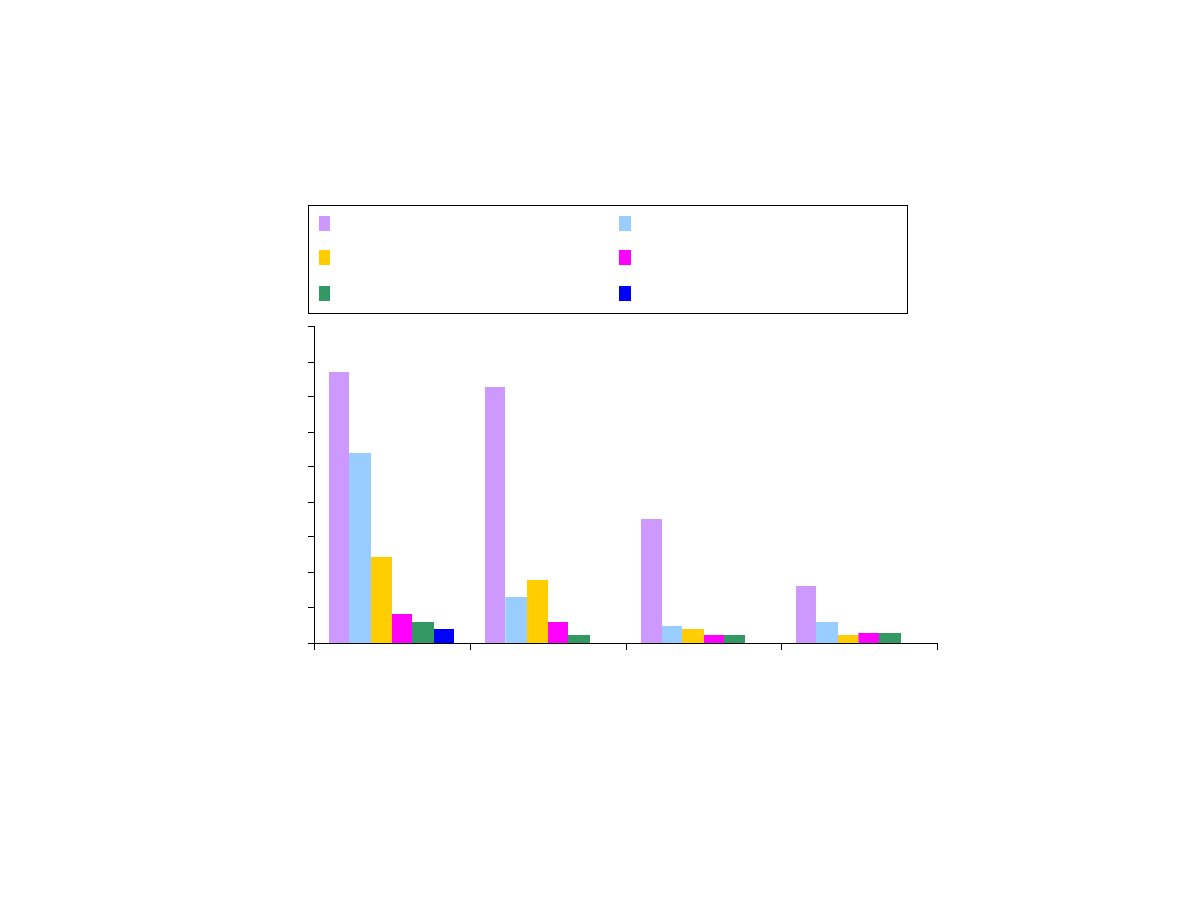
Prevalence of Abnormalities at each level of GFR
0
10
20
30
40
50
60
70
80
90
15-29
30-59
60-89
90+
Estimated GFR (ml/min/1.73 m
2
)
P
ro
p
o
rt
io
n
o
f
p
o
p
u
la
ti
o
n
(
%
)
Hypertension*
Hemoglobin < 12.0 g/dL
Unable to walk 1/4 mile
Serum albumin < 3.5 g/dL
Serum calcium < 8.5 mg/dL
Serum phosphorus > 4.5 mg/dL
*>140/90 or antihypertensive medication
p-trend < 0.001 for each abnormality
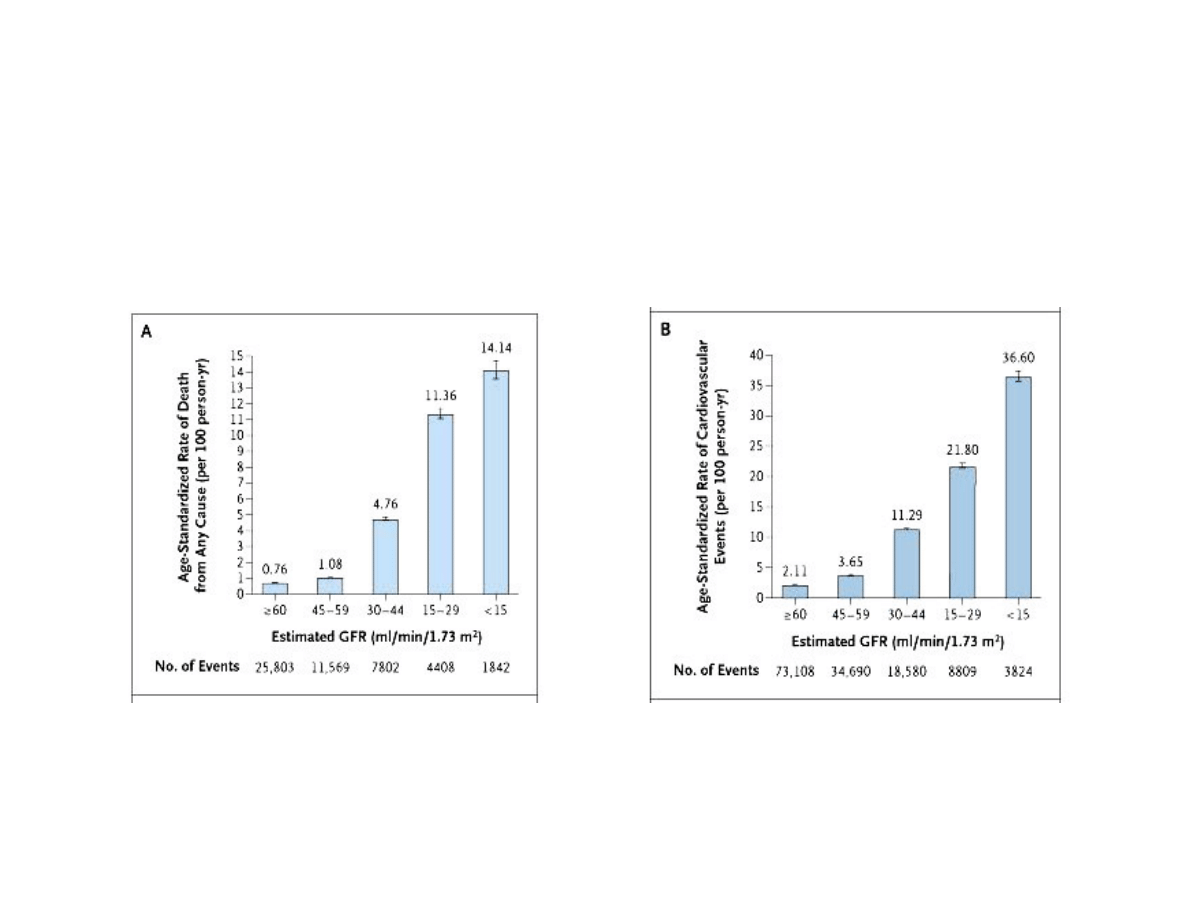
Age-Standardized Rates of Death from Any Cause
(Panel A) and Cardiovascular Events (Panel B),
According to the Estimated GFR among 1,120,295
Ambulatory Adults
Go, A, et al. NEJM 351: 1296
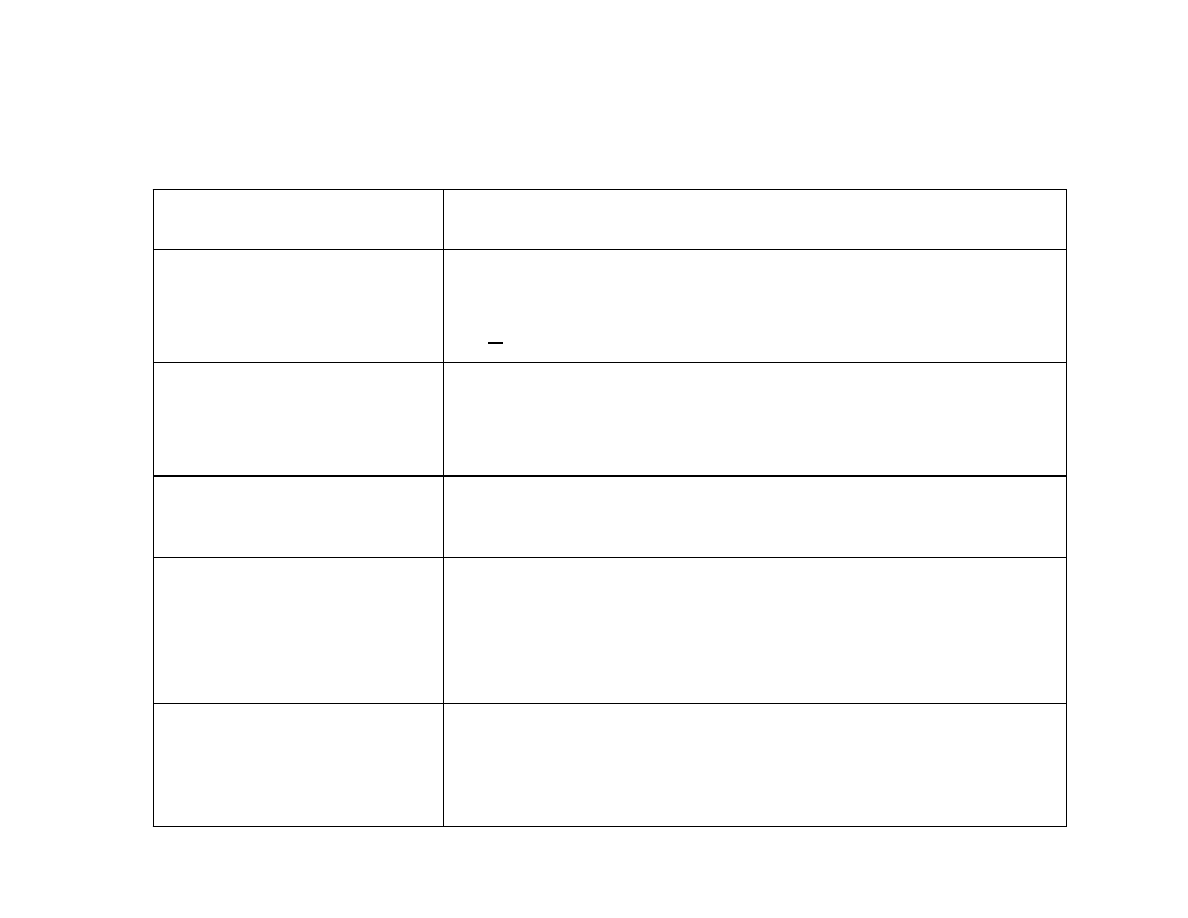
Importance of Proteinuria in CKD
Interpretation
Explanation
Marker of kidney
damage
Spot urine albumin-to-creatinine ratio >30 mg/g or
spot urine total protein-to-creatinine ratio >200 mg/g
for >3 months defines CKD
Clue to the type
(diagnosis) of CKD
Spot urine total protein-to-creatinine ratio >500-
1000 mg/g suggests diabetic kidney disease,
glomerular diseases, or transplant glomerulopathy.
Risk factor for adverse
outcomes
Higher proteinuria predicts faster progression of
kidney disease and increased risk of CVD.
Effect modifier for
interventions
Strict blood pressure control and ACE inhibitors are
more effective in slowing kidney disease
progression in patients with higher baseline
proteinuria.
Hypothesized
surrogate outcomes
and target for
interventions
If validated, then lowering proteinuria would be a
goal of therapy.
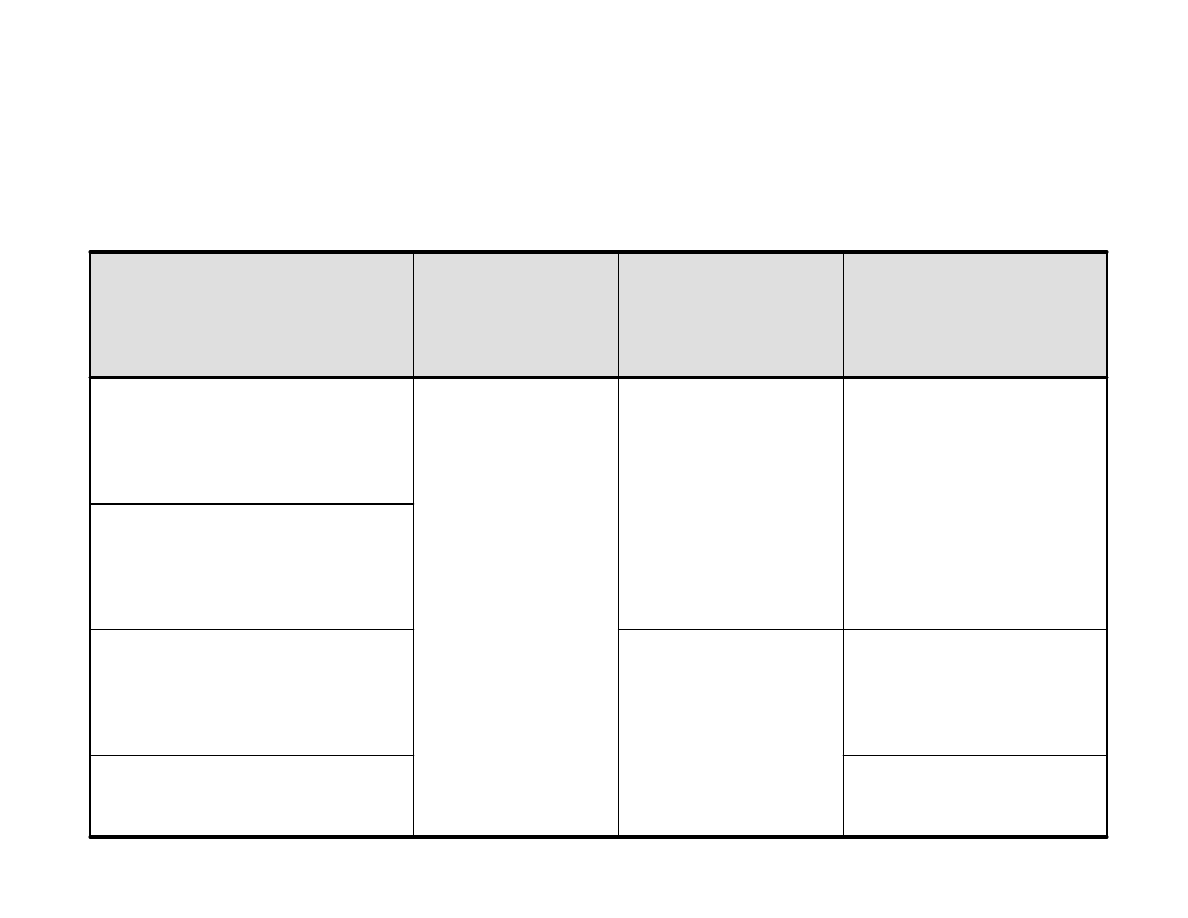
Clinical Practice Guidelines for
Management of Hypertension in CKD
CCB, diuretic, BB,
ACE inhibitor, ARB
Kidney Disease in Kidney
Transplant Recipient
Diuretic preferred,
then ACE inhibitor,
ARB, BB or CCB
None preferred
Nondiabetic Kidney
Disease with Spot Urine
Total Protein-to-
Creatinine ratio <200 mg/g
Nondiabetic Kidney
Disease with Urine Total
Protein-to-Creatinine
Ratio ≥
≥
≥
≥200 mg/g
Diuretic preferred,
then BB or CCB
ACE inhibitor
or ARB
<130/80
Diabetic Kidney Disease
Other Agents
to Reduce CVD Risk
and Reach Blood
Pressure Target
Preferred Agents
for CKD, with or
without
Hypertension
Blood Pressure
Target
(mm Hg)
Type of Kidney Disease
Treatment to Prevent Progression of CKD to
Kidney Failure
• Intensive glycemic control lessens progression from
microalbuminuria in type 1 diabetes
- DCCT, 1993
• Antihypertensive therapy with ACE Inhibitors lessens
proteinuria and progression
- Giatras, et al., 1997
- Psait, et al., 2000
- Jafar, et al., 2001
• Low protein diets lessen progression
- Fouque, et al., 1992
- Pedrini, et al., 1996
- Kasiske, et al., 1998
Meta-Analyses
Meta-Analyses

CKD is Not Being
Recognized or Treated
• Most practices screen fewer than 20% of their
Medicare patients with diabetes*
• Patients are referred late to a nephrologist,
especially African-American men
• Less than 1/3 of people with identified CKD get an
ACE Inhibitor
Kinchen, et al., 2002;
McClellan et al.,1997
*Data provided by the USRDS based on 5 percent Medicare enrollment and claims data

Who to Test for Chronic
Kidney Disease
Regular testing of people at risk
• Diabetes
• Hypertension
• Relative with kidney failure
• Cardiovascular disease
How to Test for Chronic
Kidney Disease*
In individuals with diabetes:
•
“Spot” urine albumin to creatinine ratio
In others at risk:
•
“Spot” urine albumin to creatinine ratio OR standard
dipstick
(Bouleware, et al., 2003)
•
Estimate GFR from serum creatinine using the MDRD
prediction equation
*24 hour urine collections are NOT needed. Diabetics should be
tested once a year. Others at risk testing less frequently as long as
normal.

At What Level of Creatinine Does a 65-Year-Old Diabetic, Hypertensive
White Woman Weighing 50 Kilograms Have CKD?
• 77% said:
Creatinine > 1.5 mg / dl
• Creatinine = 1.0 for GFR = 59 mL/min/1.73 m
2
GFR = 37 mL/min/ 1.73 m
2
Ccreat = 30 mL/min
Who Should be Treated for
Chronic Kidney Disease
With diabetes:
• With urine albumin/creatinine ratios more than
30mg albumin/1 gram creatinine
Without diabetes:
• With urine albumin/creatinine ratios more than
300mg albumin/1 gram creatinine corresponding
to about 1+ on standard dipstick
Or
Any patient:
• With estimated GFR less than 60 mL/min/1.73 m
2
How to Treat for Chronic
Kidney Disease
• Maintain blood pressure less than
130/80 mmHg
• Use an ACE Inhibitor or ARB
• More than one drug is usually required and a diuretic
should be part of the regimen
• Continue best possible glycemic control in individuals
with diabetes

How to Treat for Chronic
Kidney Disease
(continued)
• Refer to dietician for a reduced protein diet
• Consult a nephrologist early
• Team with the nephrologist for care if GFR is less
than 30 mL/min/1.73 m
2
• Monitor hemoglobin and phosphorous with treatment
as needed
• Treat cardiovascular risk, especially smoking and
hypercholesterolemia
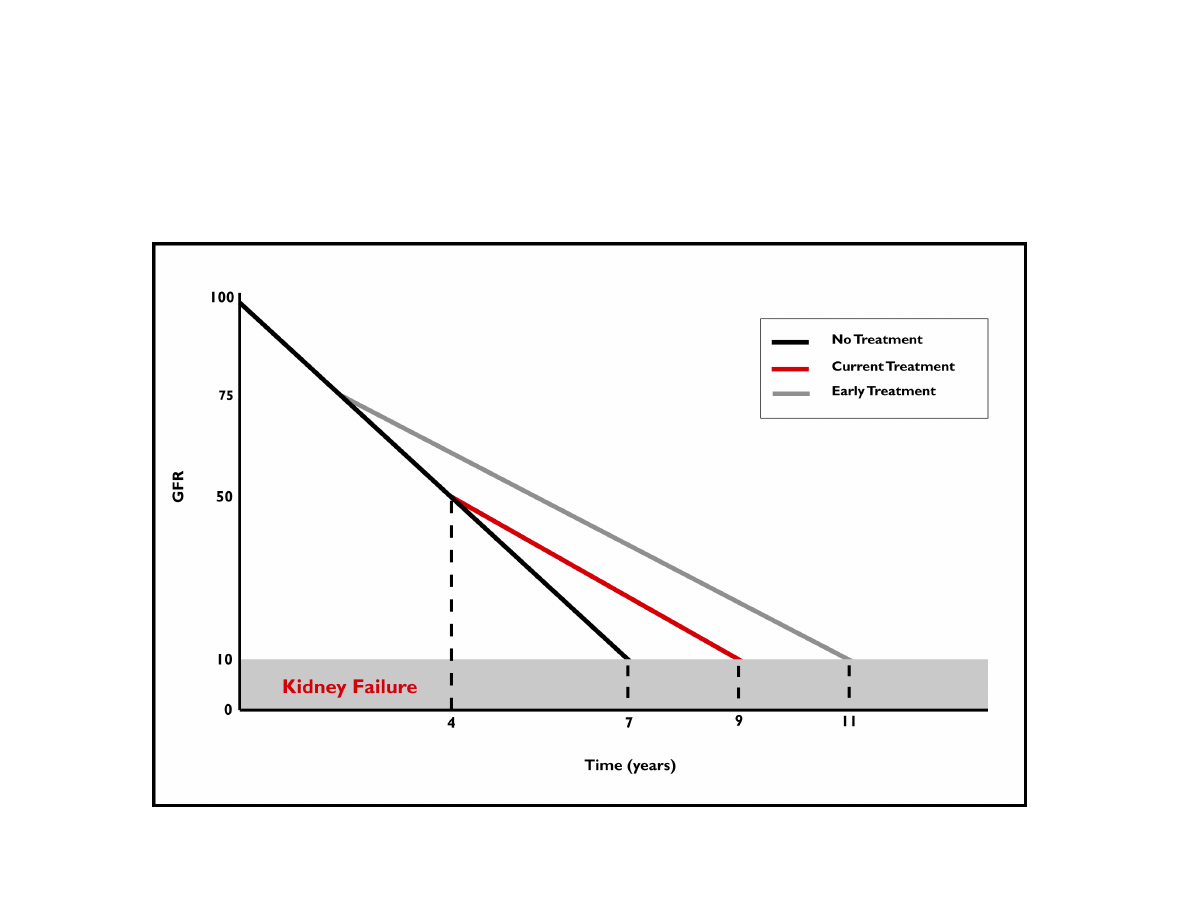
Early Treatment Makes
a Difference
Brenner, et al., 2001

Chronic Renal Failure
< 30mL/minute
decreased EPO (anemia) ***
Ca/PO4 problems (bone disease)
acidosis
hyperkalemia
Wyszukiwarka
Podobne podstrony:
patofizjologia-patomechanizmy zaburzeń układu krążenia w PNN, Ratownictwo medyczne, Ratownictwo, PAT
KZN, ONN, PNN, małopłytkowość, powikłania radio i chemioterapii
onn pnn 2013 id 335511 Nieznany
pnn
ONN I PNN, T:OSTRA NIEWYDOLNOŚĆ NEREK JAKO JEDNO ZE WSKAZAŃ DO DIALIZOTERAPII
KZN, ONN, PNN, małopłytkowość, powikłania radio i chemioterapii
Kolejno¶ć pojawiania się objawów PNN
PNN 11 03 2005 Wojcich Załuska
ONN i PNN
PNN
ONN i PNN w pediatrii
onn pnn 2005
PNN materiały, Pielęgniarstwo UM łódź, studia mgr, II semestr, piel. nefrologiczne
Lek-ONN-PNN-I-odp, medycyna, Patofizjologia
Konspekt - ONN i PNN NT NC, pięlęgniarstwo, mgr
onn pnn 2005 mi
więcej podobnych podstron