Tetracyclines
History
The development of the tetracycline
antibiotics was the result of a systemic
screening of soil specimens collected from
many parts of the world for antibiotic-
producing microorganisms. The first of these
compounds chlortetracycline was introduced
in 1948 followed by oxytetracycline and
tetracycline in 1950 and 1952 respectively.
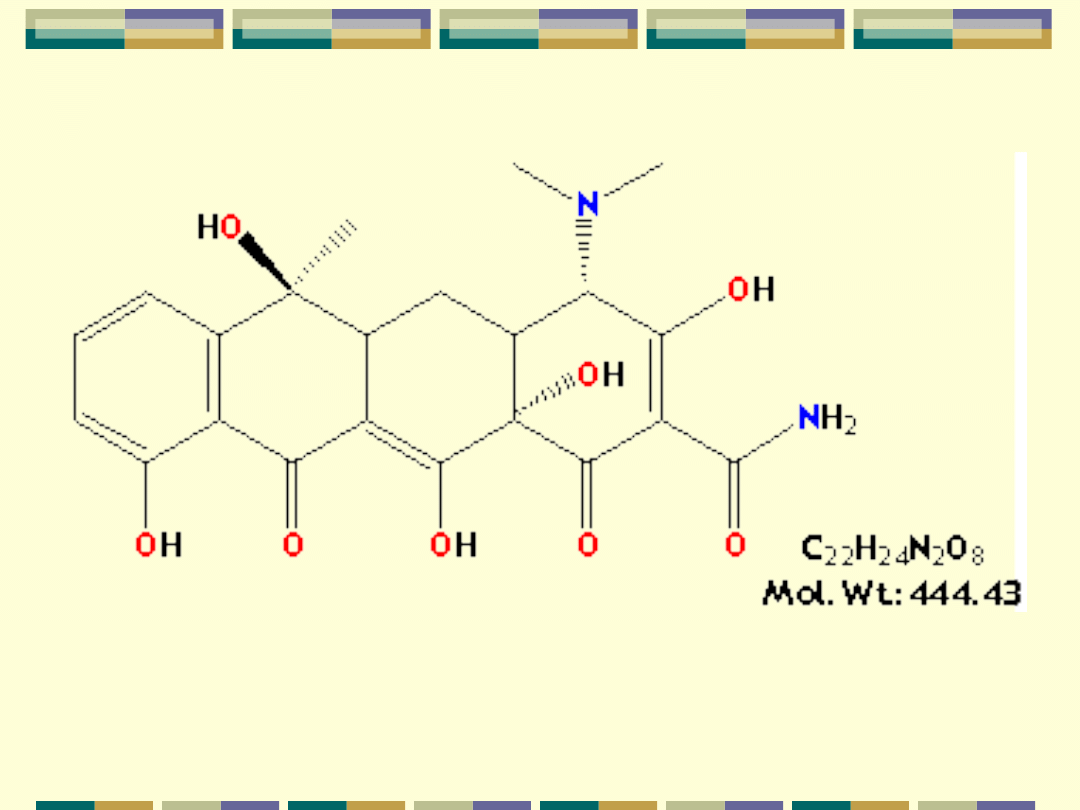
Chemistry
The basic tetracycline structure consists
of four benzene rings with various
constituents on each ring.
The crystalline bases are faintly yellow,
odorless, slightly bitter compounds. They
are only slightly soluble in water at pH 7
but they can form soluble sodium salts
and hydrochloride.
Mechanism of Action
The site of action of TET is the bacterial ribosome
and all TET function in the same manner. They are
bacteriostatic compounds. They inhibit protein
synthesis by binding specifically to the 30S
ribosome. This appears to prevent access of AA-
tRNA to the acceptor site on the mRNA-ribosome
complex; preventing the addition of AA to the
growing peptide chain.
These compounds also impair protein synthesis in
mammalian cells at high concentration. For gram
(-) bacteria, less understood for gram (+) bacteria.
Step 1 -Passive diffusion through hydrophilic
pores in the outer cell membranes.
Step 2 -Energy-dependent active transport
system that pumps all TET through the inner
cytoplasmic membrane.
Minocyline & perhaps doxycycline are more
lipophilic than the other TET and pass
directly through the lipid bilayer.
Resistance
Resistance to the TET for gram-neg and
gram-pos bacteria is mediated by
inducible plasmid [the bacteria become
resistant only after exposure to the drug].
This plasmid mediates the production of a
number of proteins that appear to affect
transport of the drug into the cell, thereby
preventing binding to the ribosomes.
Pharmacokinetics
Absorption:
All TET are adequately but incompletely
absorbed from the G.I. tract. The % of an oral
dose that is absorbed (when the stomach is
empty) is lowest for chlortetracycline (30%) and
highest for minocycline (~98-100%). Most
absorption takes place from the stomach and
upper small intestine (greater in a fasting state).
Absorption of TET is impaired by food in the
stomach, milk products, aluminum OH gels, Na+
bicarbonate, Ca++ & Mg++, and Fe++
preparations.
After a single oral dose peak
plasma concentration are achieved
in 2-4 hours.
The mechanisms responsible for
decreased absorption for
decreased absorption appear to be
chelation and an increase in
gastric pH.
Distribution
The Vd of the TET is relatively larger than that
of the body water. They are bound to plasma
protein in varying degree.
Penetration of these drugs into most tissues
and body fluids is excellent.
All TET are concentrated in the liver and
excreted by way of the bile into the intestine
from which they are partially reabsorbed
(enterohepatic circulation) Bile: serum ratio
range from 5 –lOX that of plasma.
B. CSF levels are 10 -20% of the
serum levels.
C. TET are stored in the
reticuloendothelial cells
D. TET crosses the placental barrier
and can accumulate in fetal bones,
thus delaying bone growth. They are
also excreted in breast milk.
Excretion
All the TET are excreted in the urine and the
feces, the primary route for most being the
kidney. The mechanism of renal exertion is
glomerular filtration. They will accumulate in the
body in patients with depressed renal function;
EXCEPT doxycycline -not eliminated via the
same pathways as other TET. The drug is
excreted in the feces, largely as an inactive
conjugate. Thus one of the safest of the TET for
the treatment of extrarenal infections.
Adverse Effects
TET can produce a variety of
adverse effects ranging from minor
inconvenience to life-threatening.
Gastrointestinal
TET produce GI irritation to a varying
degree in some but not all individuals.
Nausea, vomiting, burning, diarrhea
(common)
Diarrhea must be promptly
distinguished from that which results
from pseudomembranous colitis -
caused by overgrowth of clostridium
difficile ( can be life-threatening)
A. Normal -loose stools do not contain blood or
leukocytes
B. Pseudo membranous colitis -severe diarrhea,
fever, stools containing shreds of mucous
membrane and large # of neutrophils. CI. difficile
produces a toxin which is cytotoxic to mucosal cells.
TET like other antimicrobial agents administered
orally may lead to development supra infections,
usually due to strains of bacteria or yeast resistant
to these agents.
Hepatic Toxicity
Microscopic study of the liver reveals
fine vacuoles, cytoplasmic changes and
an increase in fat. Pregnant women are
particularly sensitive to TET -induced
hepatic damage. Jaundice ( increased
UREA) azotemia, acidosis, shock. (in
pregnant women experiencing
pyelonephritis can be fatal)
Renal Toxicity
TET may aggregate uremia in patients
with renal disease by I protein
synthesis - increased azotemia.
Fanconi Syndrome -observed in
patients after taking outdated and
degraded TET. - clinical picture -nausea,
vomiting, polyuria, polydipsia, acidosis,
proteinuria, glycosuria
Effects on TEETH
Children receiving long-or short term
therapy with TET may develop brown
discoloration of the teeth. The drug
deposits in the teeth and bones probably
due to its chelating property and the
formation of a TET -calcium
orthophosphate complex. This
discoloration is permanent. Avoid giving
to pregnant women and children under the
age of 8.
Other effects
Hyersensitivity Rxn -Rash, hives with
itching, itching anaphylactic rxn
( decrease in BP, increase in HR,
release of histamine, etc.)
Photoxicity -1 darkening of skin &
sunburn when patient exposed to
sunlight
Effects on Microbial
Agents
The TET possess a wide range of
antimicrobial activity against gram-positive
and gram-negative bacteria. These drugs
are primarily bacteriostatic. Only
multiplying microorganisms are affected.
Minocycline is usually the most active
followed by doxycycline then TET and
oxytetracycline (least active). Strains
inhibited by 4 ug/ml or less at TET are
considered sensitive.
Therapeutic Uses
The TET has been used extensively both for
the treatment of infections diseases. Both
uses have resulted in f bacterial resistance
to these drugs. Thus the number of
indications for the use of TET has declined.
1. TET should not be used in pregnant
women and children under 8.
2. Should not be given to patient with
severe liver disease.
Document Outline
- Tetracyclines
- PowerPoint Presentation
- Chemistry
- Slide 4
- Mechanism of Action
- Slide 6
- Resistance
- Pharmacokinetics Absorption:
- Slide 9
- Distribution
- Slide 11
- Excretion
- Adverse Effects
- Gastrointestinal
- Slide 15
- Hepatic Toxicity
- Renal Toxicity
- Effects on TEETH
- Other effects
- Effects on Microbial Agents
- Therapeutic Uses
Wyszukiwarka
Podobne podstrony:
TETRACYKLINY
tetracykliny
06 TETRACYKLINY STREPTOGRAMINY
TETRACHLOREK WEGLA, BHP KARTA CHARAKTERYSTYKI SUBSTANCJI NIEBEZPIECZNEJ
1,1,2,2 Tetrachloroetan
tetracykilny(1), Farmacja, Farmakologia
tetracykliny
Aminoglikozydy, tetracykliny itd[1]
W 43 Chloramfenikol, tetracykliny, antybiotyki
(12) Makrolidy, Linkozamidy, Aminoglikozydy, Tetracykliny, Chloramfenikol, Antybiotyki, inne(1) ppt
tetracykliny chinolony gp
12 tetracyklinyid 13630
tetracykliny, Lekarski, FARMAKOLOGIA, 1. semestr, 1sem
TETRACHLOROETEN, BHP KARTA CHARAKTERYSTYKI SUBSTANCJI NIEBEZPIECZNEJ
TETRACYKLINY(1)
więcej podobnych podstron