1/99
MedSlides.com 1
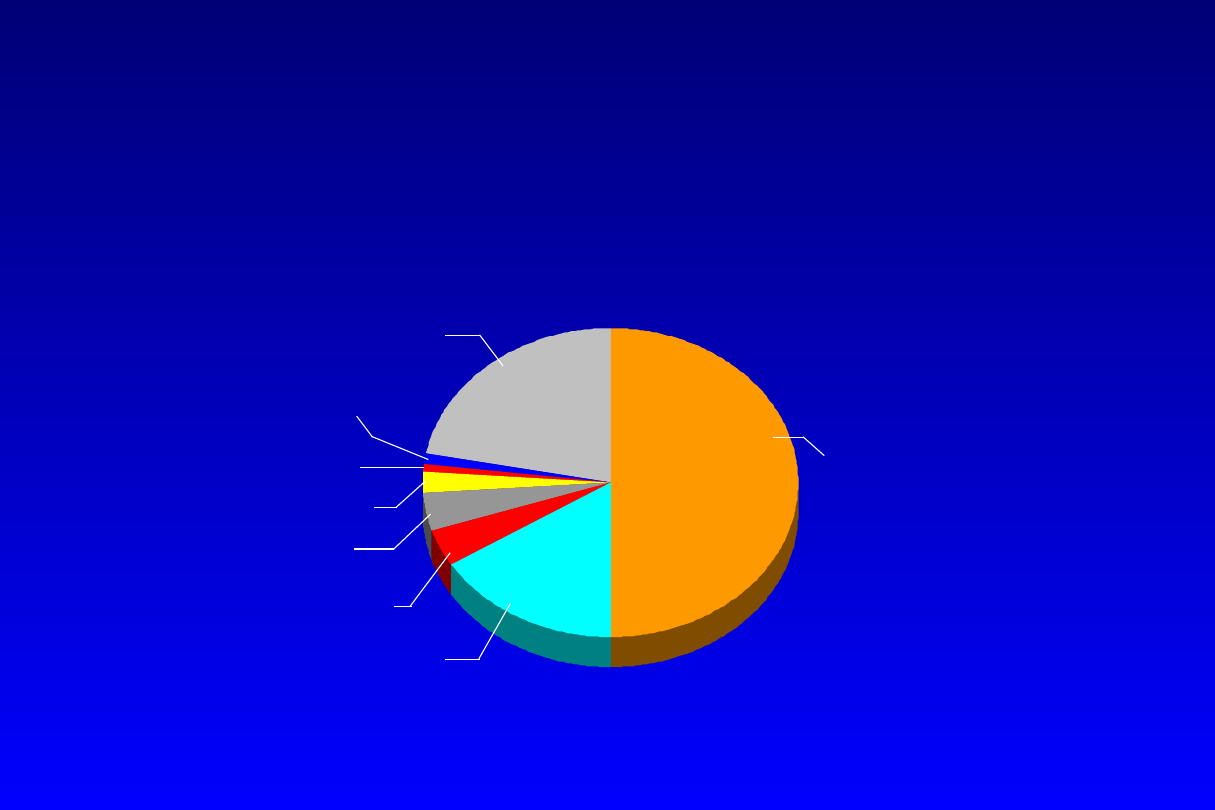
50% Coronary Heart Disease
1%
Congenit
al
Heart
Defects
1%
Rheumatic
Fever/
Rheumatic
Heart
Disease
4%
Congestive
Heart
Failure
2%
Atheroscleros
is
4% High Blood
Pressure
22% Other
Coronary Heart Disease:
Despite Advances, Still the #1 Killer
Percentage Breakdown of Deaths From Cardiovascular
Diseases
United States: 1995 Mortality, Final Data
16%
Stroke
American Heart Association
1998 Heart and Stroke Facts:
Statistical Update

1/99
MedSlides.com 2
Epidemiology
• Coronary artery disease remains the
single leading killer in the Western
world
• In the United States
–
13.5 million individuals with CAD
–
1.5 million myocardial infarctions / year
–
500,000 fatal MIs
–
estimated economic toll of $ 90 billion in
1997
Am J Cardio 1998; 1U-2U

1/99
MedSlides.com 3
Risk Factors in Primary
Prevention
National Cholesterol Education Program
Adult Treatment Panel Guidelines
Positive Risk Factors
• Age: 45 yr in men; 55 yr, or premature menopause without ERT, in
women
• Family history of premature CAD: MI or sudden death before age 55 yr
in father or other male first-degree relative, or before age 65 yr in
mother or other female first-degree relative
• Current cigarette smoking
• Hypertension: 140/90 mm Hg, or on antihypertensive medication
• Low HDL-C <35 mg/dL
• Diabetes mellitus
Negative Risk Factor
• High HDL-C: 60 mg/dL
NHLBI; September 1993
1/99
MedSlides.com 4
Castelli WP. Am J Med. 1984;76:4-12
Gotto AM Jr, et al. Circulation.
1990;81:1721-1733
1
0
-y
e
a
r
C
H
D
d
e
a
th
ra
te
(D
e
a
th
s
/1
0
0
0
)
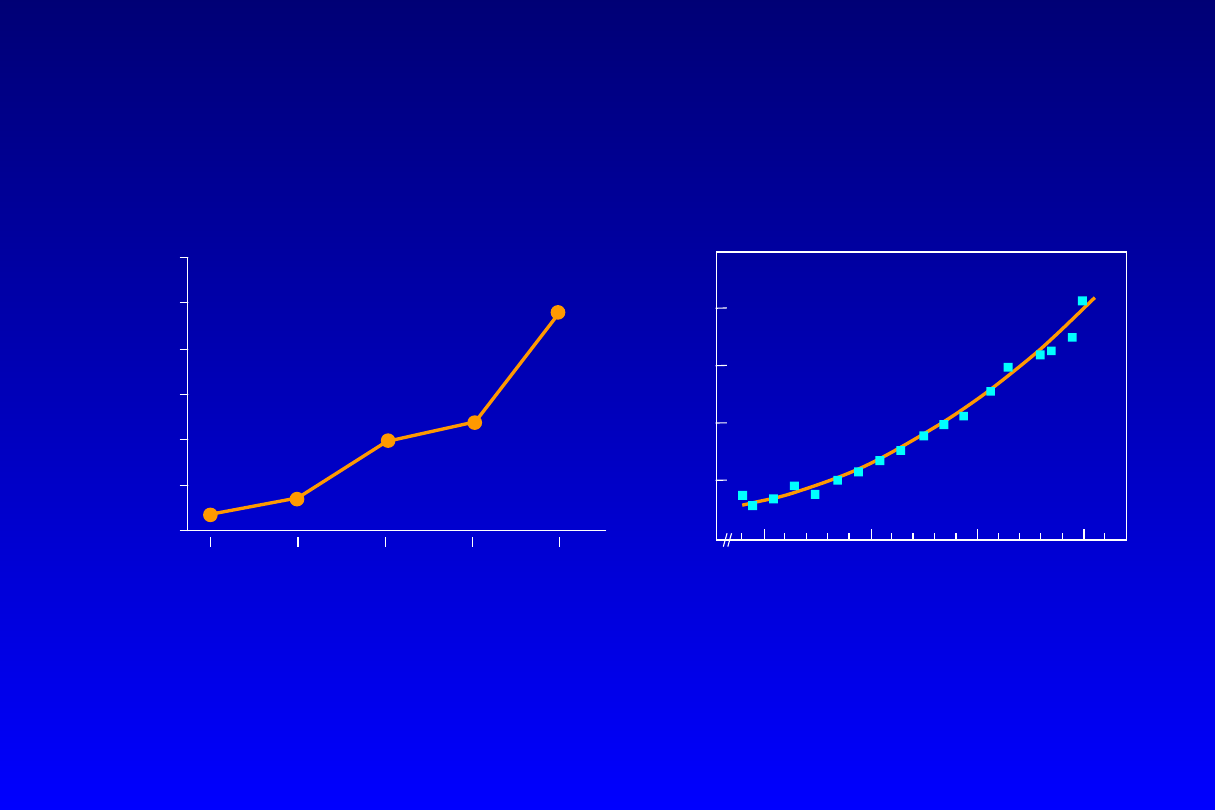
Serum cholesterol (mg/dL)
1% reduction in total cholesterol
resulted in a 2% decrease in CHD
risk
(MRFIT) (n=361,662)
150
200
250
300
0
50
40
30
20
10
0
25
50
75
100
125
150
C
H
D
i
n
d
ic
a
ti
o
n
s
p
e
r
1
0
0
0
Each 1% increase in total cholesterol
level is associated with a 2% increase
in CHD risk
Serum cholesterol (mg/100 mL)
Framingham Study (n=5209)
20
4
205-
234
235-264
265-
294
29
5
Relationship Between Cholesterol and CHD
Risk Epidemiologic Trials
1/99
MedSlides.com 5
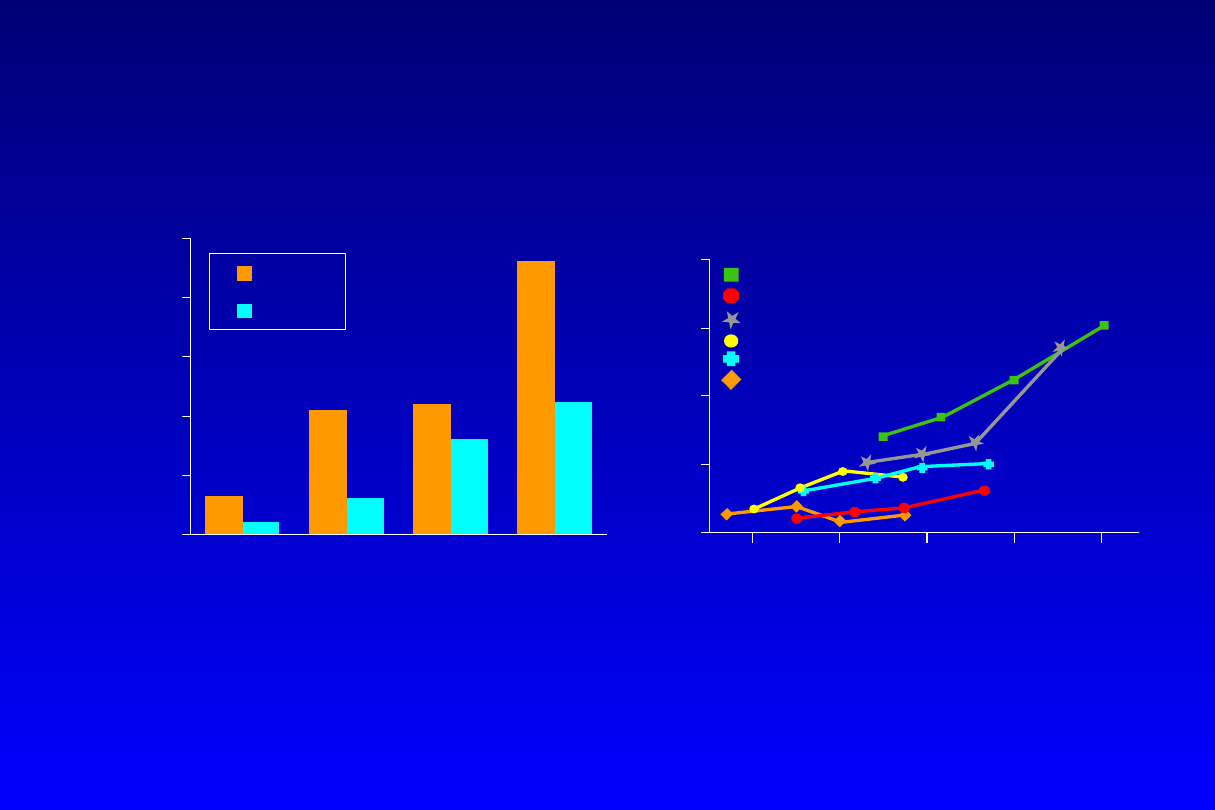
Relationship Between Cholesterol and CHD
Risk Epidemiologic Trials
Wakugami K, Iscki R, Kimura Y, et al. Japanese Circulation
Journal. 1998;62:7-14.
Verschuren WMM, Jacobs DR, Bloemberg BPM, et al. JAMA.
1995;274:131-136
C
u
m
u
la
ti
v
e
i
n
c
id
e
n
c
e
o
f
A
M
I
p
e
r
1
0
0
,0
0
0
s
c
re
e
n
e
d
s
u
b
je
c
ts
i
n
2
y
e
a
rs
0
100
200
300
400
500
Men
Women
Cumulative incidence of acute myocardial
infarction (AMI) increased with the level of
serum cholesterol
Serum cholesterol (mg/dL)
Range 167
168-191
192-217
218
Mean
149.3
179.8
203.7
245.3
Okinawa, Japan
C
H
D
m
o
rt
a
li
ty
r
a
te
s
(
%
)
Using linear approximation, a 20-
mg/dL increase in total cholesterol
corresponded to a 17% increase in
mortality risk
Serum cholesterol (mg/dL)
Seven Countries Study
†
125
175
225
275
325
0
10
20
30
40
Northern Europe
Southern Europe, Mediterranean
United States
Serbia
Southern Europe, Inland
Japan

1/99
MedSlides.com 6
Coronary Artery Disease
Risk Reduction
• For every
1%
reduction in total cholesterol, there is
a
2%
decrease in coronary artery disease
incidence
• meta-analysis by Law & coworkers (500,000 men
and 18,000 ischemic events)
age 40
1 : 5 %
age 50
1 : 4 %
age 60
1 : 3 %
age > 70
1 : 2 %
BMJ 1994:308:367-372

1/99
MedSlides.com
alkohol a miażdżyca
• umiarkowane spożycie - spadek ryzyka sercowo-naczyniowego
w porównaniu z abstynentami lub pijącymi dużo
• „francuski paradoks” - Francuzi jedzą dość dużo tłuszczów
nasyconych, ale piją też dużo wina - ryzyko sercowo-
naczyniowe podobne jak w krajach śródziemnomorskich,
mniejsze niż w USA
• wino, piwo czy alkohole wysokoprocentowe?
• czerwone wino: działanie przeciwutleniające,
naczyniorozszerzające, przeciwzakrzepowe (m. in.
rezweratrol, kwercytyna)
• być może chodzi nie o samo spożycie alkoholu, ale o styl życia

1/99
MedSlides.com
HRT a miażdżyca
•
badania epidemiologiczne i obserwacyjne - korzyść z
HRT
•
brak potwierdzenia korzyści z HRT w randomizowanych
próbach klinicznych
- badanie HERS (Heart and Estrogen-Progestin
Replacement Study) - brak wpływu HRT na
występowanie incydentów sercowo-naczyniowych
- badanie ERA (Estrogen Replacement and
Atherosclerosis Trial) - brak korzyści z HRT w ocenie
angiograficznej (MLD)

1/99
MedSlides.com
Chlamydia pneumoniae a miażdżyca
• podwyższone miano przeciwciał we krwi pacjentów z
miażdżycą i w próbkach uzyskanych podczas
aterektomii wieńcowej
• brak potwierdzenia związku przyczynowo-skutkowego
pomiędzy zakażeniem chlamydiami a niestabilnymi
zespołami wieńcowymi
• badanie ROXIS - stosowanie roksytromycyny w
niestabilnych zespołach wieńcowych (po 8 miesiącach
- zmniejszenie częstości występowania incydentów
klinicznych)
1/99
MedSlides.com10
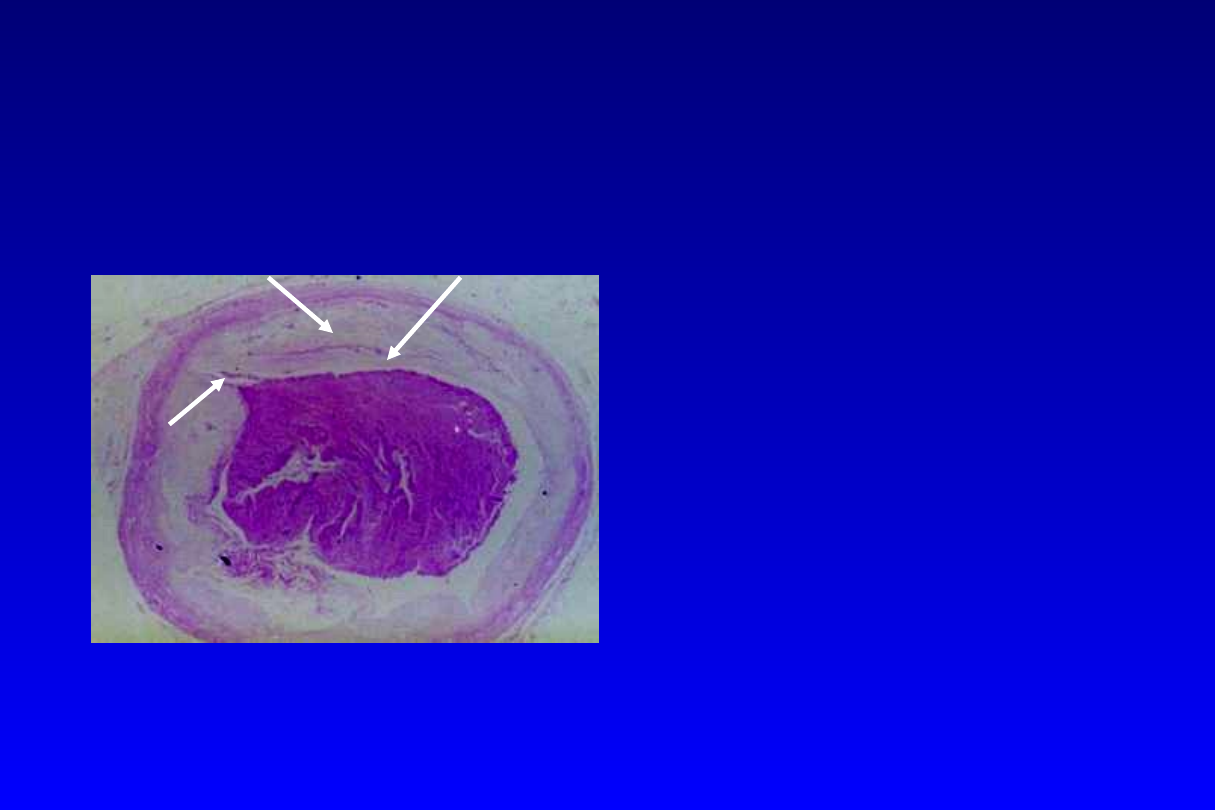
Mechanisms of plaque
rupture
• Vulnerable plaque
– a thin fibrous cap
– large lipid-rich core
– high concentration of
inflammatory cells
• Culprit lesion (FATS)
– a small group of all
plaques (1 in 8) have
substantial lipid core,
causing majority (8 of
9) of cardiac events
Lipid core
Fibrous cap
plaque
rupture
thrombus

1/99
MedSlides.com11
Culprit Lesions
severity of coronary stenoses at initial
angiogram 30.2 months before myocardial
infarction in 329 patients
0
5
10
15
20
25
30
35
40
45
50
<50
50-75
>75
Diameter Stenosis (%)
P
a
ti
e
n
ts
(
%
)
Am J Cardio 1997;80(9A):2I-10I

1/99
MedSlides.com12
Lipid Lowering Therapy
• reduce the risk of
– total mortality
– non-fatal myocardial infarction
– myocardial revascularization procedures
– stroke or transient ischemic attack
• slow CAD progression
• regression of atherosclerotic lesions
1/99
MedSlides.com13
Primary Prevention
Secondary Prevention
Statin Mega Trials
1994 - 4S (Scandinavian Simvastatin)
1995 - WOSCOP (West of Scotland)
1996 - CARE (Chol and Recurrent Event)
1997 - Post-CABG Trial
1998 - LIPID Trial (long-term intervention)
1998 - AFCAPS / TexCAPS

1/99
MedSlides.com14
Statin Prevention Studies
Primary prevention
WOSCOPS
Men only with no documented MI
H
(n = 6,595)
AFCAPS/TexCAPS Men and women with no clinical CAD
NM
(n = 6,605)
Secondary prevention
4S
Men and women with previous CAD
H
(n = 4,444)
CARE
Men and women with a history of MI
NM
(n = 4,159)
LIPID
Men and women with a history of MI
NH
(n = 9,014)
and/or unstable angina pectoris
(Total cholesterol:
H
=high,
NM
=normal to mild,
NH
=normal to high)
1/99
MedSlides.com15
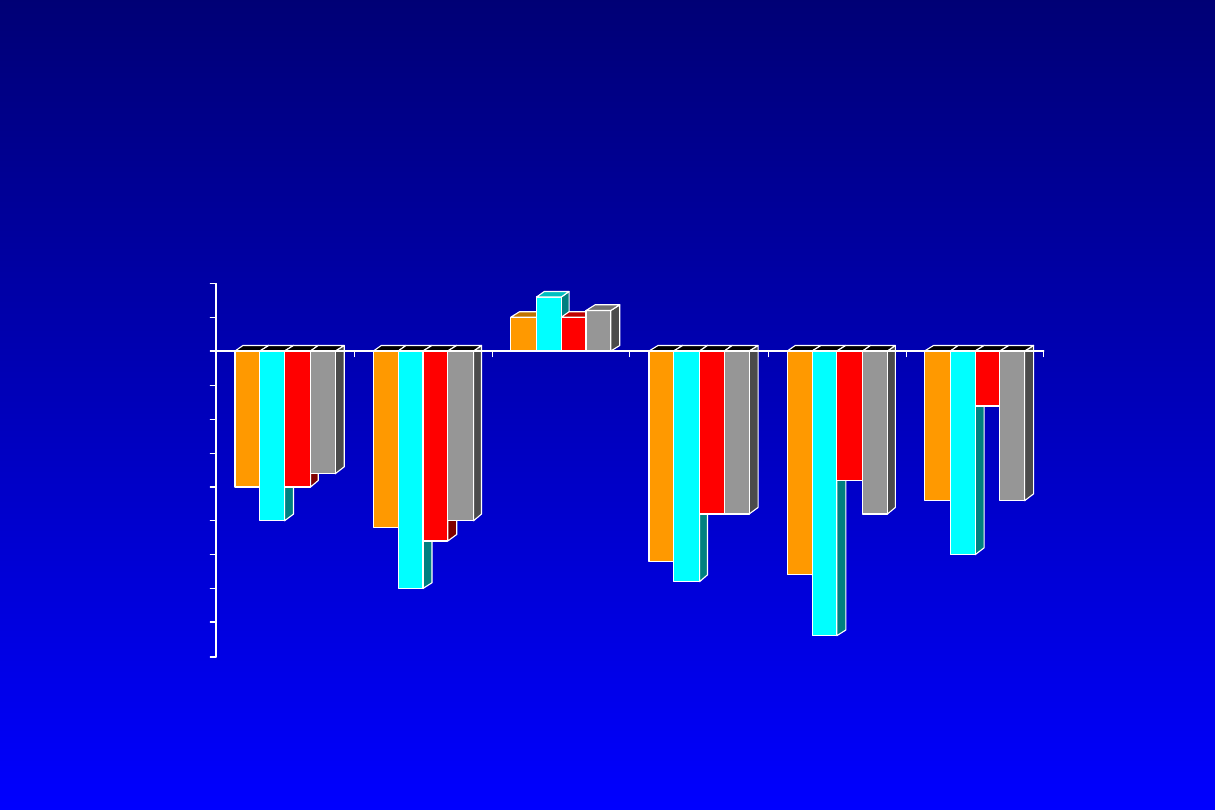
Statin Prevention Trials
-20
-25
-20
-18
-26
-35
-28
-25
5
8
5 6
-31
-34
-24
-24
-33
-42
-19
-24 -22
-30
-8
-22
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
5
10
WOSCOPS
4S
CARE
LIPID
TC
LDL-C
HDL-C
Nonfatal
MI/CAD
Death
CAD
Death
All-Cause
Mortality
*
*
1/99
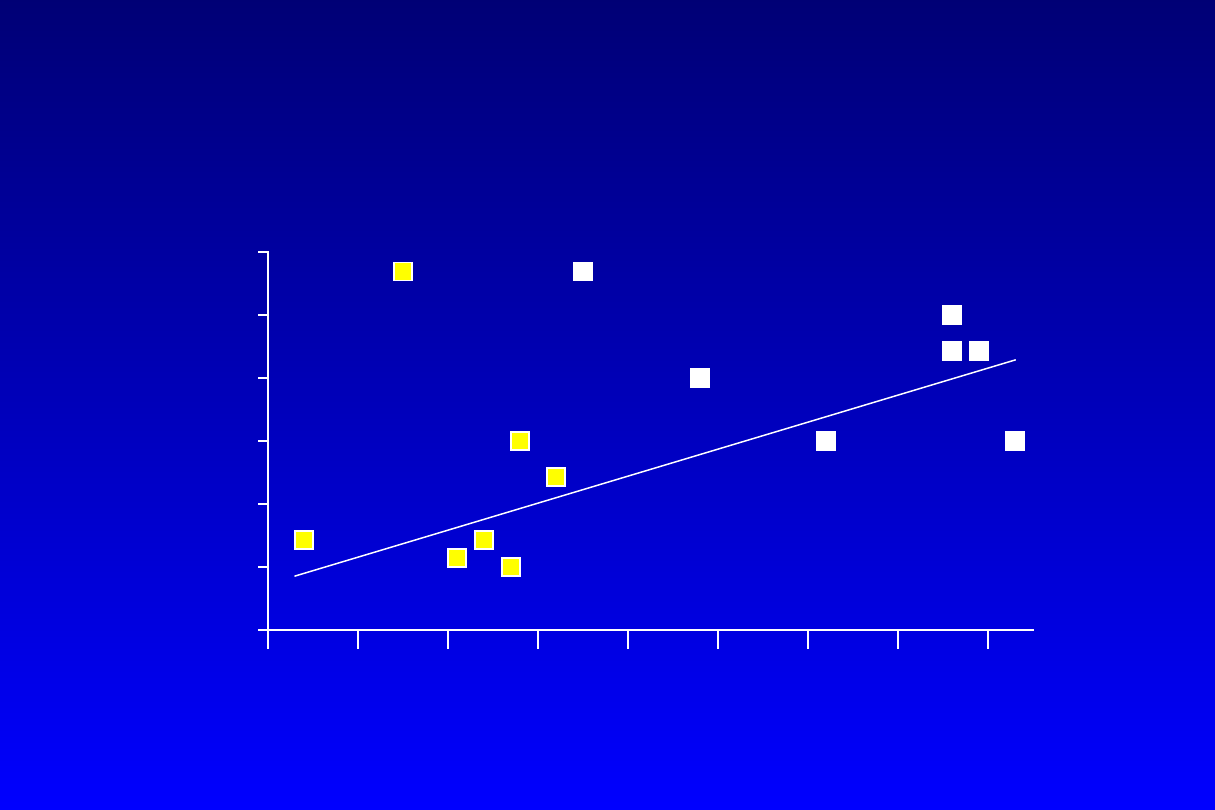
MedSlides.com16
Statin Prevention Trials
decrease in clinical events with
lower LDL-C
LDL-C Achieved (mg/dL)
100 110 120
90
130 140 150 160 170 180 190 200
0
5
10
15
20
25
30
E
v
e
n
t
R
a
te
(
%
)
AFCAPS
CARE
AFCAPS
WOSCOPS
WOSCOPS
CARE
LIPID
LIPID
4S
4S
Treatment
Placebo
1
0
prevention
2
0
prevention
1/99
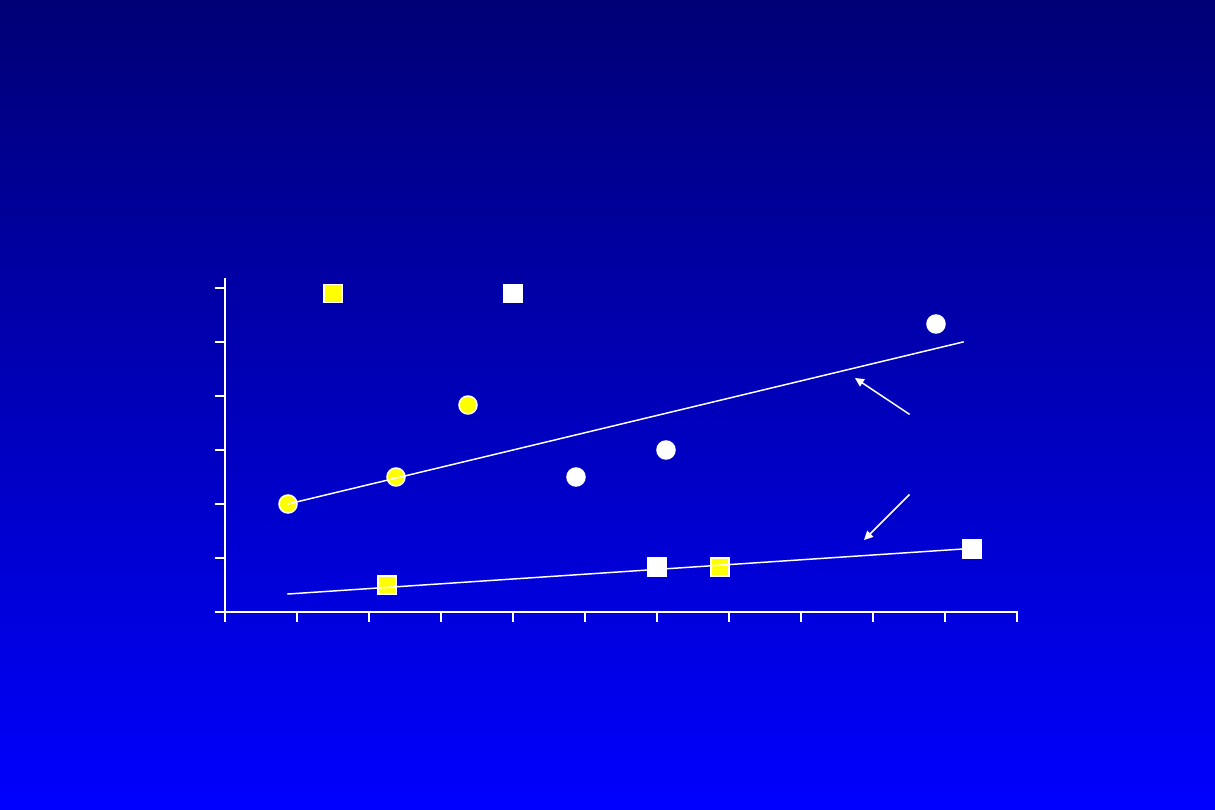
MedSlides.com17
Angiographic Statin Trials
treatment predictive of MLD change
100
90
110
120
130
140
150
160
170
LDL-C Achieved (mg/dL)
0.01
0.02
0.03
0.04
0.05
0.06
0.00
Pr
o
g
re
ss
io
n
(
M
LD
d
e
cr
e
a
se
)
(m
m
/y
)
Treatment
Placebo
MARS
LCAS
MAAS
REGRESS
CCAIT
PLAC I
MARS
MAAS
LCAS
PLAC I
CCAIT
REGRESS
Curr Opin Lipidol 1997;8:354-361

1/99
MedSlides.com18
Primary Prevention Trials
Effect on Nonfatal MI or CAD Death
LDL-C 5 year Event Rate
Trial
Base / Rx / % statin / placebo / RRR
ARR /
NNT
WOSCOPS
192 159
26%
5.3% 7.5%
29%
2.2%
46
(N=6,595)
Pravastatin 40
AFCAP/
150 115
25%
3.5% 5.5%
37%
2.0%
50
TexCAPS
(N=6,605)
Lovastatin 20-40
RRR = relative risk reduction
ARR = Absolute risk reduction
NNT = 1/ARR = # need to treat to prevent 1 event
Arch Intern Med 1998

1/99
MedSlides.com19
WOSCOPS
West of Scotland Prevention Study
Determine whether long-term therapy with pravastatin to
decrease LDL-C would decrease the incidence of first
acute major event
NEJM 1995;333:1301-1307
• Design: double-blind,
pravastatin (40 mg/day)
• Patients: 6,595 men, age 45-64, no history of MI. Baseline
lipids: TC 221 mg/dL, LDL-C 150 mg/dL, triglyceride 158 mg/dL
• Results: At 4.9-year follow-up, total cholesterol reduction was
20% greater than placebo, LDL by 26%, triglycerides by 12%,
HDL increased by 5%.
Major coronary event (nonfatal MI
and CAD death) was reduced by 31%
(p<.001). Risk for
overall mortality was reduced by 22% (p=0.051).

1/99
MedSlides.com20
AFCAPS / TexCAPS
Air Force / Texas Coronary Atherosclerosis
Prevention Study
Determine whether long-term therapy with lovastatin to decrease
LDL-C would decrease the incidence of first acute major event
(unstable angina, fatal and nonfatal MI, sudden cardiac death)
JAMA 1998;279:1615-1622
• Design: double-blind,
lovastatin (20-40 mg/day), LDL-C goal <110
mg/dL
• Patients: 6,605 adults age 73 (5,608 , 997), baseline lipids: TC 221
mg/dL, LDL-C 150 mg/dL, triglyceride 158 mg/dL
• Results: At 5.2-year follow-up, total cholesterol reduction was 18.4%
greater than placebo, LDL by 25%, triglycerides by 15%, HDL increased
by 6%.
First acute coronary event was reduced by 37%
(p<.001).
Significant reduction also seen in secondary endpoints:
revascularization, 33%; unstable angina, 32%; fatal and nonfatal MI,
40%; fatal and nonfatal coronary events, 25%.

1/99
MedSlides.com21
Secondary Prevention Trials
Effect on Nonfatal MI or CAD Death
LDL-C 5 year Event Rate
Trial
Base / Rx / % statin / placebo / RRR
ARR /
NNT
4S (1994)
188 122
35%
19.4% 27.9%
34%
8.5%
12
simvastatin
CARE (1996)
139 98
32%
10.2% 13.2%
24%
3.0%
34
pravastatin
LIPID (1998)
150 112
25%
12.3% 15.7%
23%
3.4%
30
pravastatin
Arch Intern Med 1998

1/99
MedSlides.com22
4S
Scandinavian Simvastatin Survival Study
To determine whether long-term cholesterol reduction with
simvastatin will reduce overall mortality in post-myocardial
infarction (MI) and angina patients with hypercholesterolemia
• Design:
simvastatin (20-40 mg/day)
• Patients: 4,444 pts with CAD (MI or angina), baseline TC 212-310
mg/dL
• Results: Average 5.4-year follow-up. Simvastatin reduced TC by 25%,
LDL-C by 35%, triglyceride by 10%; HDL increased by 8%.
Risk of
total mortality was reduced by 30%
(p<0.00001). Other benefits
of treatment included the reduction of coronary mortality by 42%,
major coronary events by 34%, CABG/PTCA by 37%, LDL-C by 38%.
Lancet 1994; 344:1383-1389

1/99
MedSlides.com23
CARE
Scandinavian Simvastatin Survival Study
To determine whether long-term cholesterol reduction with
pravastatin will reduce overall mortality in post-myocardial
infarction (MI) patients with “average” cholesterol level.
• Design:
pravastatin (40 mg/day)
• Patients: 4,159 pts (3,583 , 576 ) with prior MI; baseline TC
<240 mg/dL (mean 209), LDL 115-174 mg/dL (mean 139)
• Results: Average 5-year follow-up. Therapy reduced TC by 20%,
LDL-C 28%, triglyceride 14%; HDL increased 5%.
Risk of major
coronary event (nonfatal MI and fatal coronary event) was
reduced by 24%
(p=0.003). There was no significant change in
overall mortality or mortality from noncardiovascular causes.
N Engl J Med 1996;335:10001-1009

1/99
MedSlides.com24
LIPID
Long-term Intervention with
Pravastatin in Ischemic Disease
Assess efficacy of treatment with pravastatin (Pravachol, Bristol
Myers Squibb) on reduction of coronary mortality and morbidity in
patients with history of myocardial infarction or unstable angina
and average or below average total and LDL cholesterol levels.
• Design: double-blind,
pravastatin (40 mg/day)
vs placebo
• Patients: 9,014 (83% ), age 31-75, baseline cholesterol 219
mg/dL (155-271), LDL-C 150 mg/dL, triglyceride 161 mg/dL
• Results: At 6.1-year follow-up, total cholesterol reduction was
18% greater than placebo (p=.001), LDL by 25%, triglycerides
by 12%, HDL increased by 6% (p=.001).
Coronary mortality
was reduced by 24%
(6.4% vs 8.3%, p<0.001). Total mortality
was reduced by 22% ( 11.0% vs 14.1%, p<0.001).
N Engl J Med 1998;339:1349-1357

1/99
MedSlides.com
populacje o dużym i małym ryzyku
liczebność populacji
10000 10000
liczba incydentów rocznie
100
10
zmniejszenie ryzyka względnego
30%
30%
korzyść z leczenia (ile incydentów mniej?)
30
3
poważne objawy uboczne
0,1% 0,1%
szkodliwość leczenia (ile powikłań?)
10
10
koszt leczenia 1 pacjenta rocznie
1
1
koszt uniknięcia jednego incydentu
333
3333
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
Wyszukiwarka
Podobne podstrony:
88 Leki przeciwreumatyczne część 2
guzy część szczegółowa rzadsze
Miazdzyca
miażdżyca1b
Stomatologia czesc wykl 12
S II [dalsza część prezentacji]
(65) Leki przeciwreumatyczne (Część 1)
Teoria organizacji i kierowania w adm publ prezentacja czesc o konflikcie i zespolach dw1
Strukturalizm i stylistyka (część II)
Biznesplan część finansowa
Czasowniki modalne The modal verbs czesc I
psychopatologia 6 podejscie systemowe czesc 2
PROCES MIAŻDZYCOWY A(1)
Alkaloidy część pierwsza
więcej podobnych podstron