
Neoplasms
Neoplasms
of Respiratory
of Respiratory
System
System

Epidemiologic data
Epidemiologic data
Number of patients:
• 1,35 million people per year on the whole world (2003);
• Global incidence in male –
35,5/100.000, in female – 12,1/100.000.
There were 215.020 patients in USA (114.690 male and 100.330
female). Incidence - 63,9/100.000 (79.4/100.000 for male,
52.6/100.000 for female). Surveillance Epidemiology and End Results
(http://www.seer.cancer.gov); 20 000 people in Poland.
In 2008, 161.840 patients died due to lung cancer in USA (death rate -
72.0/100.000 for male and 41.0/100.000 for female). In USA, 75%
patients died during 5 years from cancer diagnosis, in Poland – 86%.
The median age of diagnosis was 70 years (in 2003, in USA). 32,6%
patients was diagnosed between 65 and 74 years age.
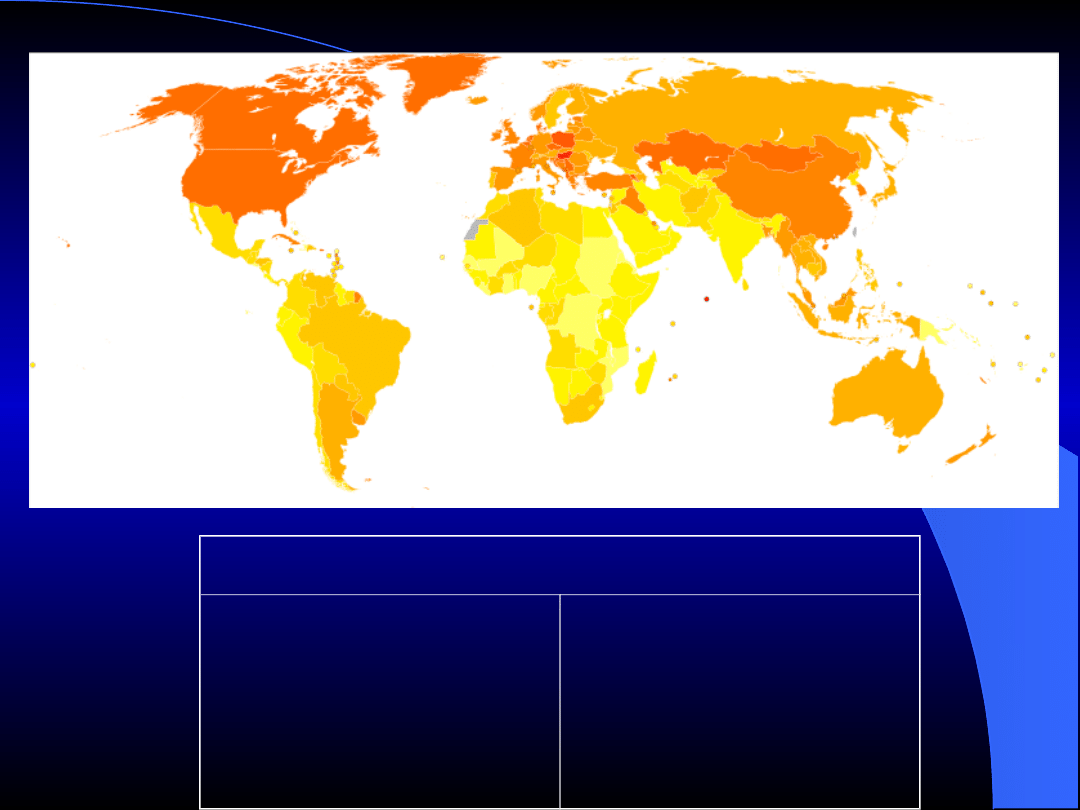
Age-standardised death rates from Trachea, bronchus,
lung cancers by country (per 100,000 inhabitants).
no data
less than 5
5-10
10-15
15-20
20-25
25-30
30-35
35-40
40-45
45-50
50-55
more than 55
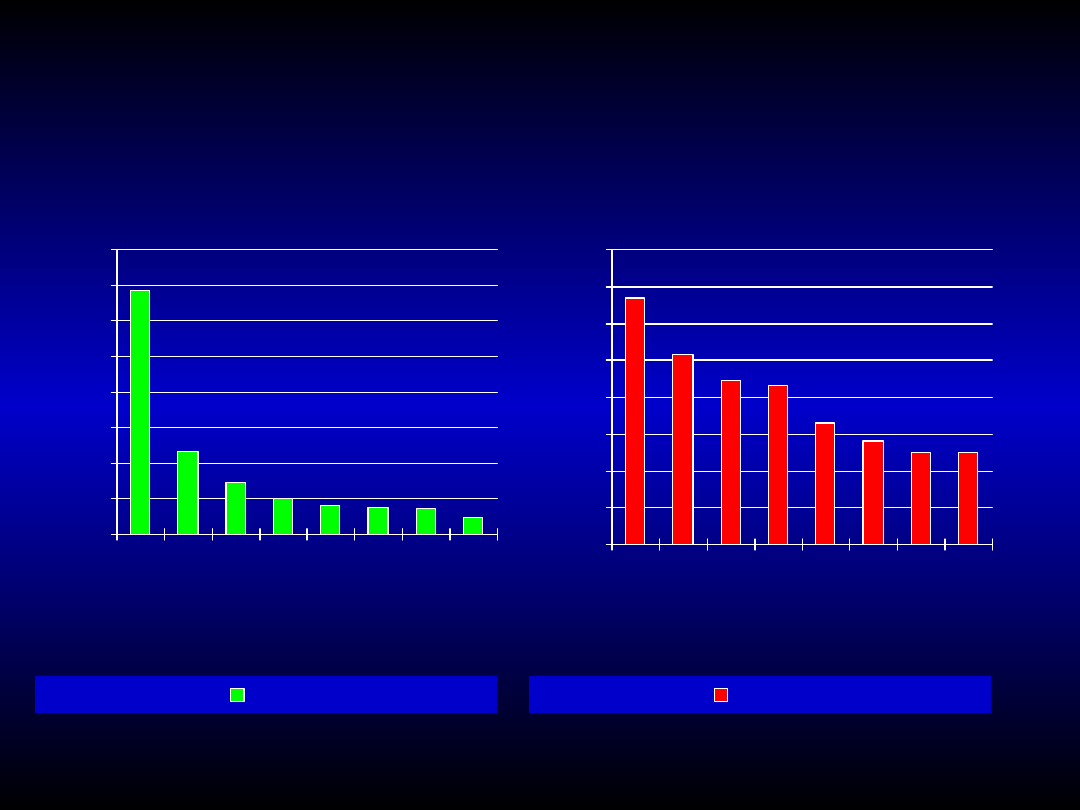
Cause of death in course of
Cause of death in course of
malignant neoplasms in Poland
malignant neoplasms in Poland
(1999)
(1999)
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
40,0
lu
ng
st
om
ac
h
co
lo
n
pr
os
ta
te
pa
nc
re
as
ur
in
ar
y
bl
ad
de
r
lar
yn
x
es
op
ha
gu
s
male
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
16,0
br
ea
st
co
lo
n
st
om
ac
h
lu
ng
ut
er
in
e
ce
rv
ix
ov
ar
iu
m
pa
nc
re
as
ga
llb
la
de
r
female
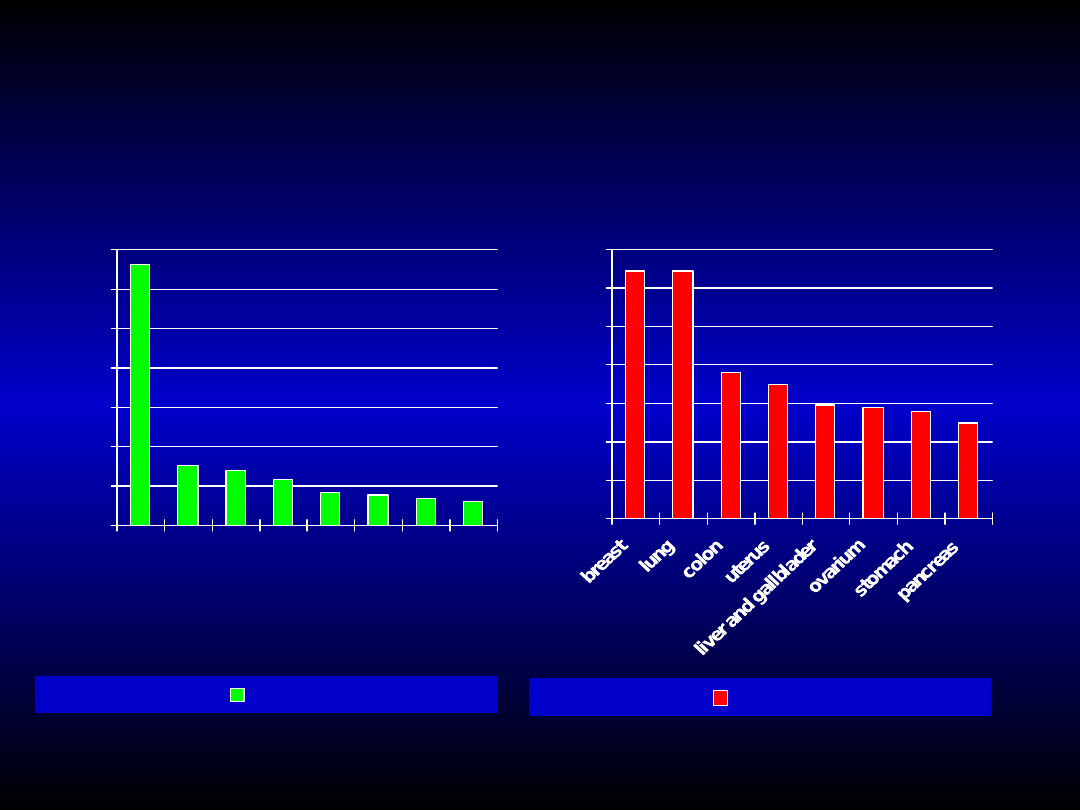
Cause of death in course of
Cause of death in course of
malignant neoplasms in Poland
malignant neoplasms in Poland
(2003)
(2003)
0,0
5,0
10,0
15,0
20,0
25,0
30,0
35,0
lu
ng
st
om
ac
h
pr
os
ta
te
co
lo
n
ur
in
ar
y
bl
ad
de
r
pa
nc
re
as
re
ct
um
a
nd
an
us
lar
yn
x
male
0,0
2,0
4,0
6,0
8,0
10,0
12,0
14,0
female
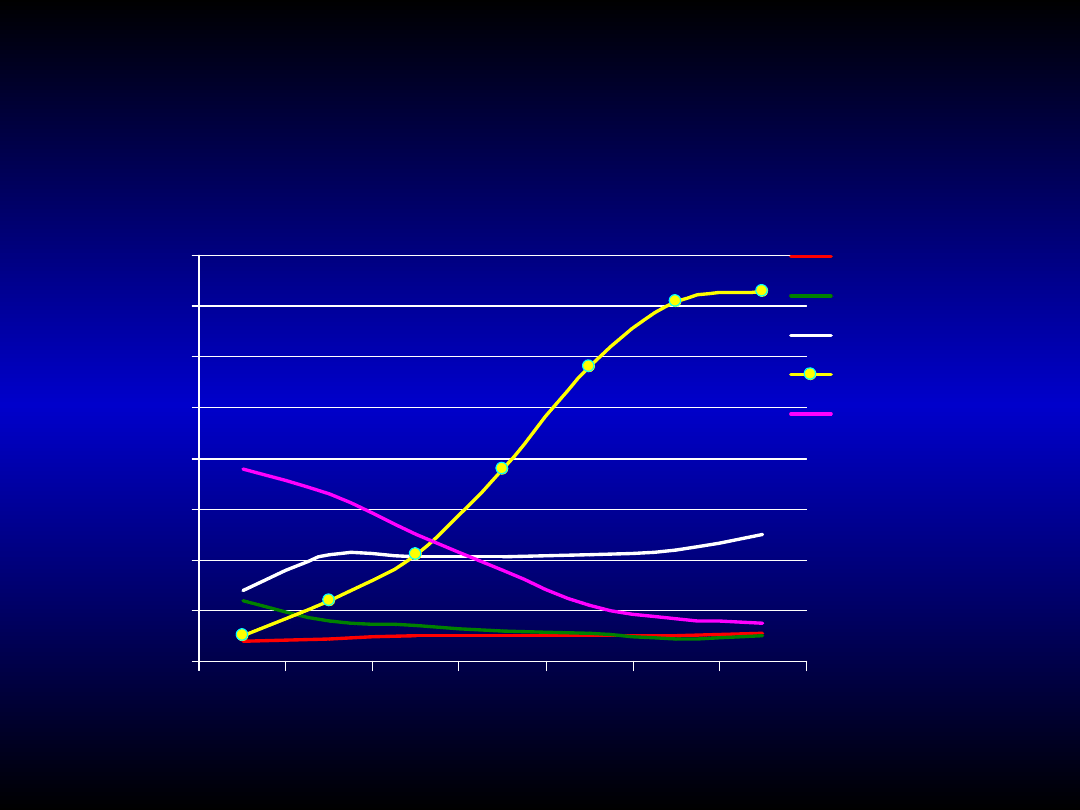
Death rate because of malignant
Death rate because of malignant
neoplasm's in male in USA
neoplasm's in male in USA
0
10
20
30
40
50
60
70
80
1930 1940 1950 1960 1970 1980 1990
p
er
1
00
0
00
esophagus
liver
prostate
lung
stomach
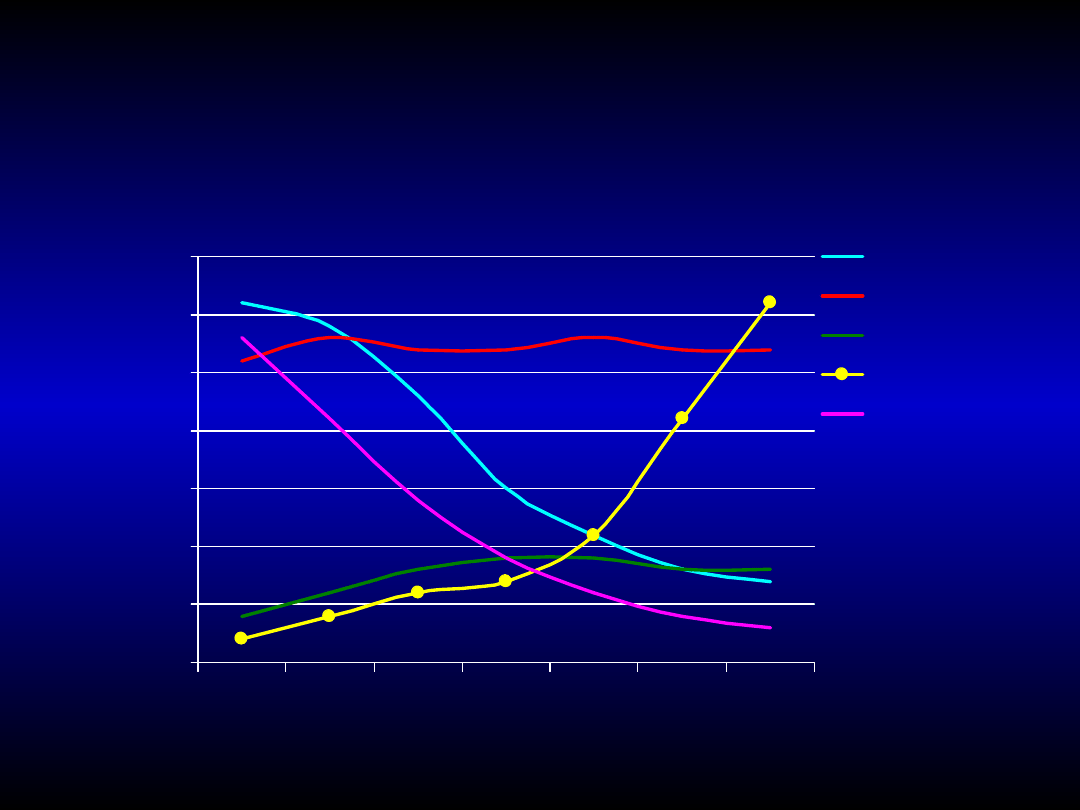
Death rate because of malignant
Death rate because of malignant
neoplasm's in female in USA
neoplasm's in female in USA
0
5
10
15
20
25
30
35
1930 1940 1950 1960 1970 1980 1990
p
er
1
00
0
00
uterus
breast
ovary
lung
stomach

Smoking (percentage of
Smoking (percentage of
population)
population)
POLAND
USA
female
27 %
30 %
male 48 %
28 %
Smoking tobacco is the major risk factor for developing lung
cancer.
Smokers have
10-25
times greater risk of lung cancer than
non-smokers.
Exposition to second-hand smoke:
1,5
times greater risk of
lung cancer.
Cigarette smoke includes more than 2000 carcinogens, e.g.
bezno[A]pirene, polyclic aromatic hydrocarbons,
nitrosamines, arsenic, hydrogen cyanide.

Additional risk factors in
Additional risk factors in
smokers
smokers
Contents of tarry substances in cigarettes.
Manner of inhaling the smoke.
Age of smoking beginning.
Age of discontinuation of smoking.
The number of cigarettes per day.
}
The
number of
pack-years

Mechanisms of smoke
Mechanisms of smoke
pathogenic activity on
pathogenic activity on
respiratory system
respiratory system
ciliotoxicity and impairement of
bronchial cleaning (bronchial
clearance);
disturbances in protease -
antiprotease balance;
abnormalities in immunological
response;
induction of chronic inflammation
state in airways;
bronchial hypersensitivity;
mutagenesis and oncogenesis.

1964 – Surgeon General’s
Report on Smoking and
Health:
• For the first time, this report
admitted official that smoking is
significant risk factor in
appearance of respiratory system
diseases.
CDC (Centres for Disease
Control):
• Smoking is in charge of more
than 80.000 death in year in USA
because of respiratory system
disease.

Environmental and
Environmental and
occupational carcinogenic
occupational carcinogenic
factors in lung cancer
factors in lung cancer
FACTORS
FACTORS
Asbestos
Asbestos
Combustion gases from
Combustion gases from
oxidization of coal,
oxidization of coal,
petroleum and soot,
petroleum and soot,
diesel engine exhaust
diesel engine exhaust
gases
gases
Radon
Radon
Arsenic
Arsenic
OCCUPATIONAL EXPOSURE
OCCUPATIONAL EXPOSURE
thermal insulation, plumbers
engineering;
stokers, steelworkers,
mechanics, miners and
machine operators, chimney
sweeps;
miners;
miners, welders, workers at
pesticide production.
Genetic factors in lug cancer
Genetic factors in lug cancer
In lung cancer cells are accumulated
many genetic alterations, such as:
Small cell
Non-small cell
lung cancer
lung
cancer
Alterations in tumor
3p deletion
3p deletion
suppressor genes
mutation in RB
mutation in p6
mutation in p53
mutation in p53
Alterations in
myc expression myc
expression oncogenes
Her-2/neu expression
mutation in ras
Bcl-2
expression Bcl-2 expression
telomerase expr. telomerase expr.

Prevention in lung cancer
Prevention in lung cancer
(National Cancer Institute Recommendation)
(National Cancer Institute Recommendation)
Smoking cessation – 30-50% reduction
of death rate is noticed after 10 years
from smoking cessation.
• Zyban (bupropione hydrochloride – 150 mg) –
selective
inhibitor
of
neuronal
uptake
of
noradrenaline and dopamine.
• Chantix (verenikline) – partial agonist of nicotinic
receptors.
Early detection of high risk of lung
cancer (genetic predisposition) and
effective diagnosis of non-invasive
forms.

Interruption of precancerous conditions
(atypical adenomatous hyperplasia –
AAH, diffuse spontaneous proliferation of
neuroendocrine cells, progressive
dysplasia, cancer in situ).
Secondary chemoprevention in developed
lung cancer (adjuvant chemotherapy in
patients after tumor resection).
Primary chemoprevention (tocopherols,
beta-carotenes, retinoids, diet).
Prevention in lung cancer
Prevention in lung cancer
(National Cancer Institute Recommendation)
(National Cancer Institute Recommendation)

Diet in lung cancer
Diet in lung cancer
Protective activity (antioxidative
Protective activity (antioxidative
activity)
activity)
-carotenes;
vitamin C;
vitamin A.

Lung cancer
Lung cancer
Lung cancer is malignant neoplasm derived
from airway epithelium cells (bronchi,
bronchiole, alveoli).
There are two types of lung cancer: small cell
lung cancer (SCLC) and non-small cell lung
cancer (NSCLC).
88% of primary lung cancers:
• squamous cell lung cancer (cornnifying or non-cornifying);
• small cell lung cancer;
• lung adenocarcioma (with brochioloalveolar adenocarcinoma subtype);
• giant cell carcinoma (anaplastic cell carcinoma).

Frequency of lung cancer in
Frequency of lung cancer in
USA
USA
Histological type
Frequency
5-years
survival
Lung adenocarcinoma
32% 17%
Brochioloalveolar adenocarcinoma 3%
42%
Squamous cell lung cancer
29% 15%
Microcellular lung cancer
18% 5%
Macrocellular lung cancer
9%
11%
Carcinoid (typical or atypical)
1%
83%
Salivary gland carcinoma 0,2% 39% - 48%
Mucoepithelioid carcinoma
Adenoid cystic carcinoma
Sarcocarcinoma
0,1% 30%

Histopathological diagnosis of lung cancer
Histopathological diagnosis of lung cancer
is the basic factor, which decide of kind of
is the basic factor, which decide of kind of
treatment. It qualifies tumor as a small cell
treatment. It qualifies tumor as a small cell
lung cancer (lat.
lung cancer (lat.
carcinoma
carcinoma
microcellulare
microcellulare
)
)
or one of types of non-small cell lung
or one of types of non-small cell lung
cancer.
cancer.
At the moment of the diagnosis and the
At the moment of the diagnosis and the
first symptoms occurrence, small cell lung
first symptoms occurrence, small cell lung
cancer is usually systemic disorder with
cancer is usually systemic disorder with
distant metastases by lymph and blood
distant metastases by lymph and blood
vessel. Time of duplicate of tumor size is
vessel. Time of duplicate of tumor size is
only 55 days. Therefore, SCLC may be treat
only 55 days. Therefore, SCLC may be treat
by chemo- or/and radiotherapy.
by chemo- or/and radiotherapy.

Lung cancer - clinical
Lung cancer - clinical
symptoms
symptoms
Only 5-15% of patients have no
symptoms at the moment of lung
cancer diagnosis.

The symptoms connecting with
The symptoms connecting with
intrabronchial growth of primary
intrabronchial growth of primary
tumor
tumor
couth (45-75%);
shortness of breath and chronic fatigue (30-50%);
haematoptysis (27-57%);
unilateral whistling rales, wheezing breath, stridor;
weight loss for no known reason (8-70%);
lung inflammation because of bronchus occlusion
(fever, productive couth);
chest pain.

occlusion of a bronchus or trachea lumen;
dysphagia;
symptoms of lung abscess (squamous cell carcinoma and
giant cell carcinoma);
periodic reversible nerve paralysis with hoarseness (5-20%);
phrenoplegia with elevation of phrenic dome;
infiltration of pericardium and heard, cardiac tamponade
(squamous cell carcinoma and small cell lung cancer);
pleural effusion (adenocarcinoma and giant cell lung
cancer);
hypoxemia and respiratory failure.
Symptoms connecting with tumor
Symptoms connecting with tumor
spreading in the chest area
spreading in the chest area

Horner’s Syndrome – sympatic nerve paralysis
with, retraction of eyeball, tonic pupil, ptosis
of upper eyelids and hypohidrosis;
Pancoast’s Syndrome – symptoms of the lung
apex tumor (commonly squamous cell
carcinoma) with damage of C8-Th2 spinal
nerves, generation of omalgia and destruction
of first and second costal bones;
Superior caval vein syndrome with swelling of
the face and neck - 5% of patients.
Symptoms connecting with
Symptoms connecting with
tumor spreading in the chest
tumor spreading in the chest
area
area

Symptoms of lung cancer
Symptoms of lung cancer
metastases
metastases
metastases to lymph nodes – compression syndromes;
metastases to bones – ostalgia and pathologic
fracture;
metastases to liver – hepatocellular damage with
icterus and liver insufficiency;
metastases to central nervous system – deficiency
signs and cephalgia;
metastases to bone marrow – pancytopaenia and
leucoertroblastosis.

Paraneoplastic syndromes (10-
Paraneoplastic syndromes (10-
30%)
30%)
there are no connection between
paraneoplastic syndrome and tumor size
or distant metastatic presence;
paraneoplastic syndromes are associated
with SCLC and giant cell carcinoma;
paraneoplastic syndrome are dependent
on production by cancer cells
polypeptide hormones, antibodies or
immunomodulators such as TNF-α,
prostaglandins.

Paraneoplastic syndromes
Paraneoplastic syndromes
neoplasm's cachexy (30% of patients) and fever
dependent on TNF-α release;
disturbances of coagulation (profound venous
embolothrombotic disease, wandering
embolism, DIC syndrome). Tissue factor is
produced by neoplastic cells;
hypercalcaemia and hypophosphataemia due to
ectopic production of parathormon or peptide
similar to parathormon (PTHrH);
paraneoplastic neuro- and myopathy. Subacute
peripheral sensory neuropathy;
hypertrophic pulmonary osteoarthropathy with
clubbed fingers.

suspicion of neoplastic disease on the
basis of full medical history of patient
(symptoms, coexistent diseases,
general condition, state of nutrition,
smoking and family history) and
physical examination;
planning of additional examination
(blood cell count, blood coagulation,
biochemistry, electrolytes, tuberculin
test, chest-X-ray examination.
The role of general practicioner
The role of general practicioner
in diagnosis of lung cancer
in diagnosis of lung cancer

Chest-X-ray examination
Chest-X-ray examination
localisation of change
localisation of change
probability of diagnosis
probability of diagnosis
central squamous cell carcinoma small cell lung
cancer
peripheral
giant cell carcinoma lung
adenocarcinoma
disseminated or
brochioloalveolar
multifocal
carcinoma infiltration
pleural effusion
lung adenocarcinoma
hylar
lymphadenopathy

Diagnosis of lung cancer
Diagnosis of lung cancer
Chest-X-ray sensitivity is 70-80%
“
“
Malignancy trait” in chest-X-ray examination
Malignancy trait” in chest-X-ray examination
weak separation of change;
lack of central calcification;
duplication time < 18 months;
size > 3 cm;
accompanying atelectasis, pneumonia and/or
lymphadenopathy
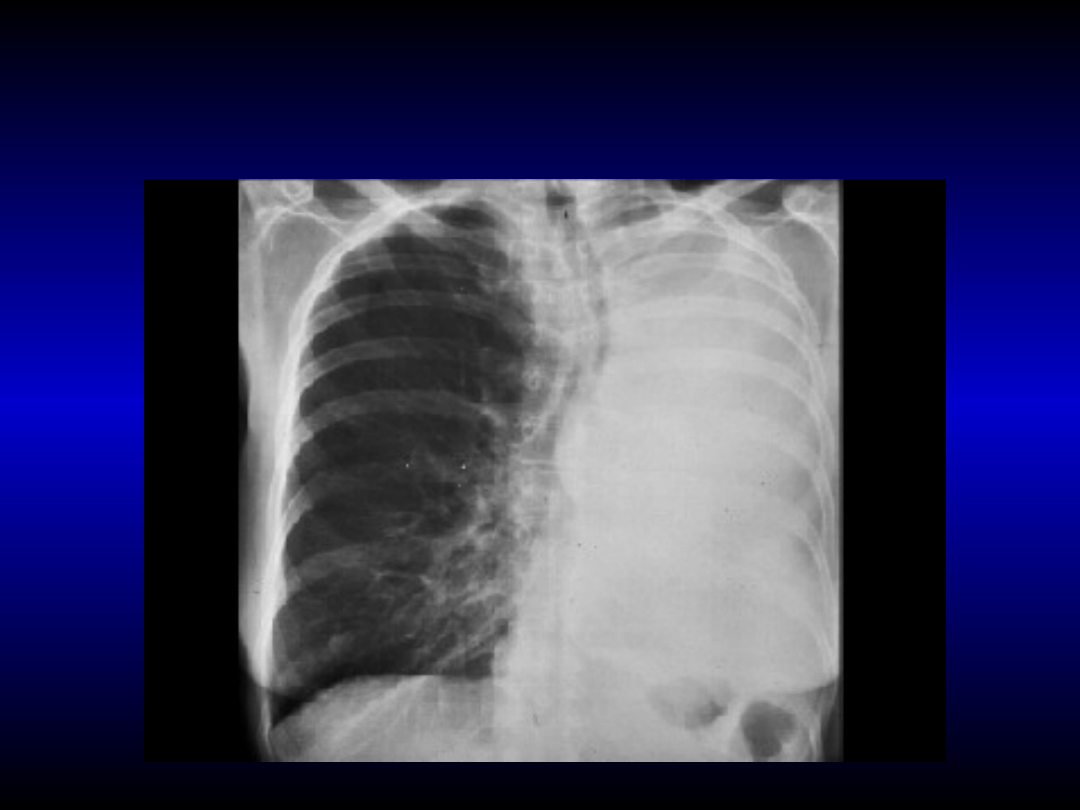
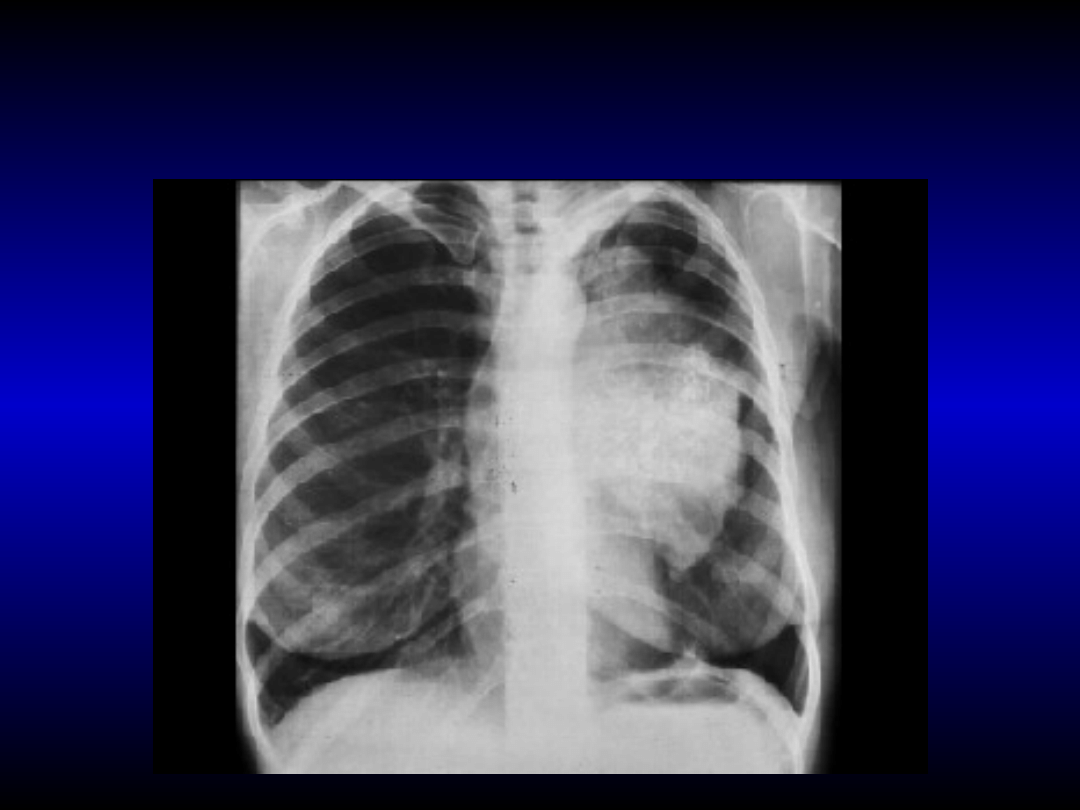
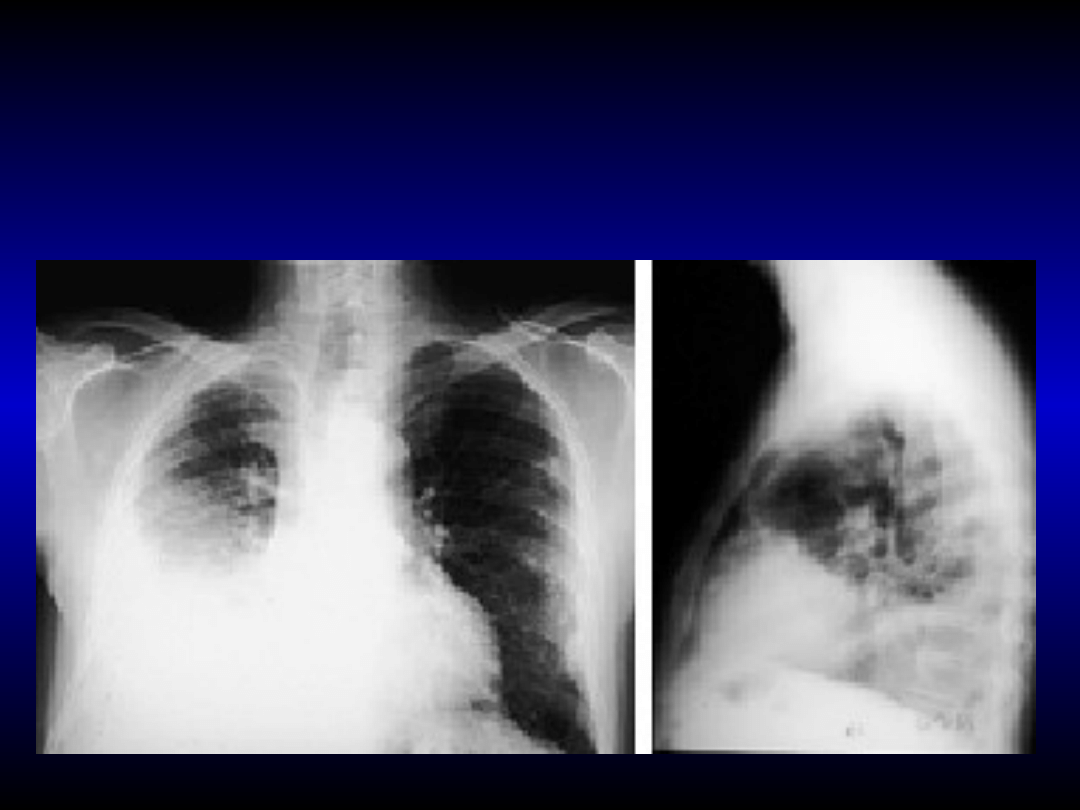
Squamous cell carcinoma shutting left main
Squamous cell carcinoma shutting left main
bronchus. Trachea and main vessels are
bronchus. Trachea and main vessels are
shifted to the left
shifted to the left
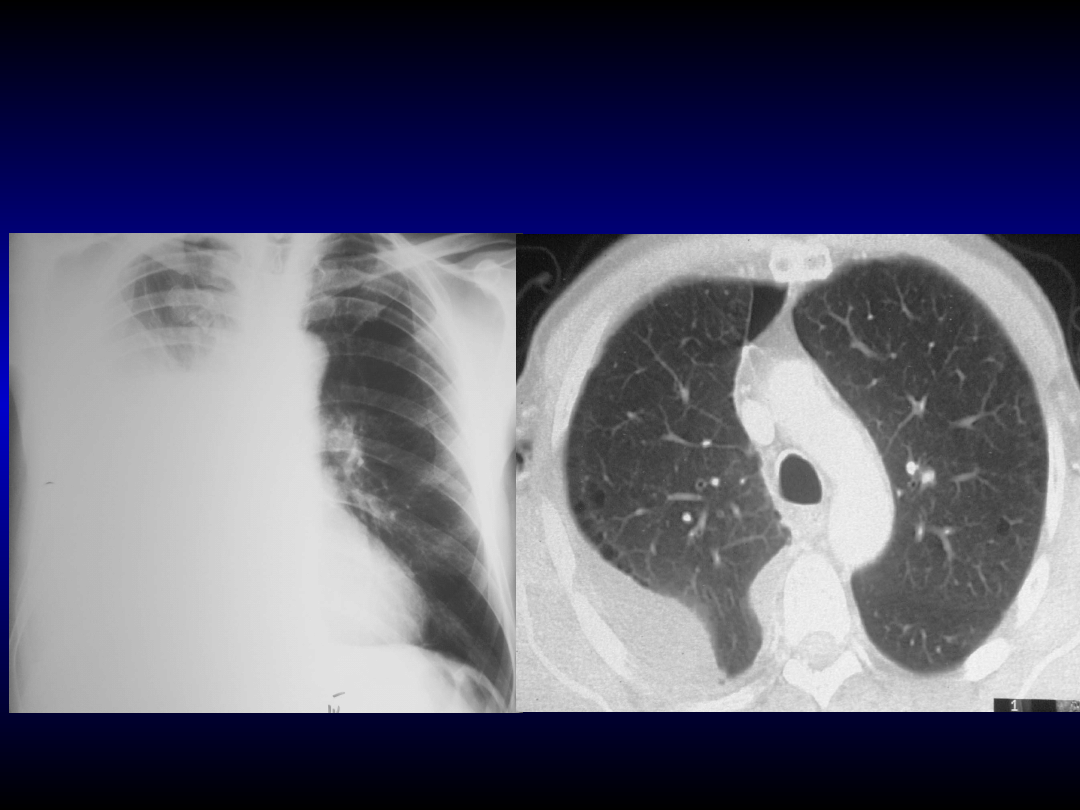
Pleural ephusion in course of
Pleural ephusion in course of
lung adenocarcinoma
lung adenocarcinoma
Infiltration of pleura and lung inflammation
Infiltration of pleura and lung inflammation
causing by neoplasm occlusion of bronchus
causing by neoplasm occlusion of bronchus
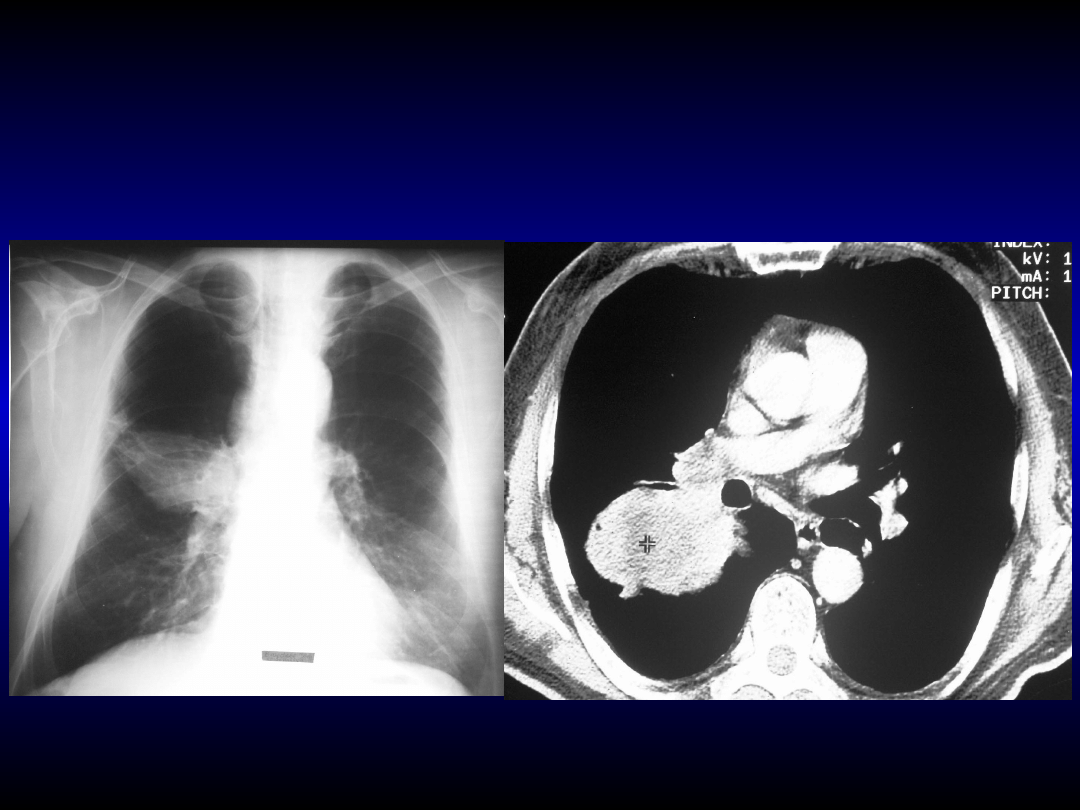
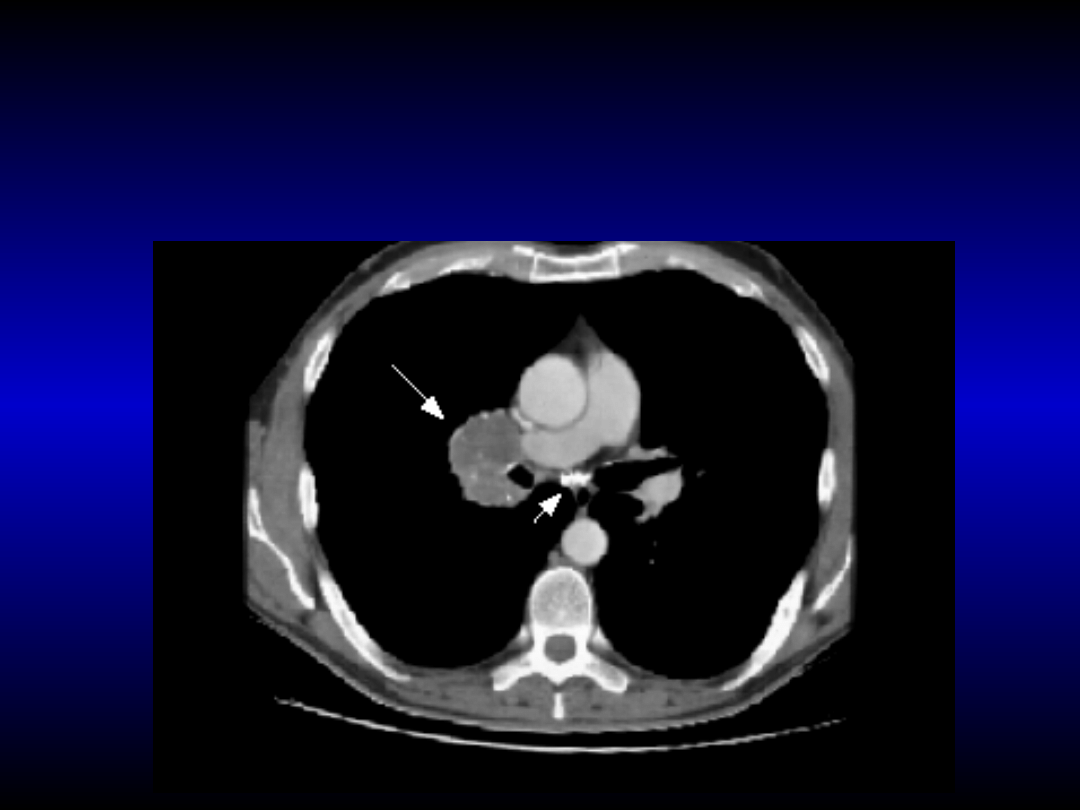
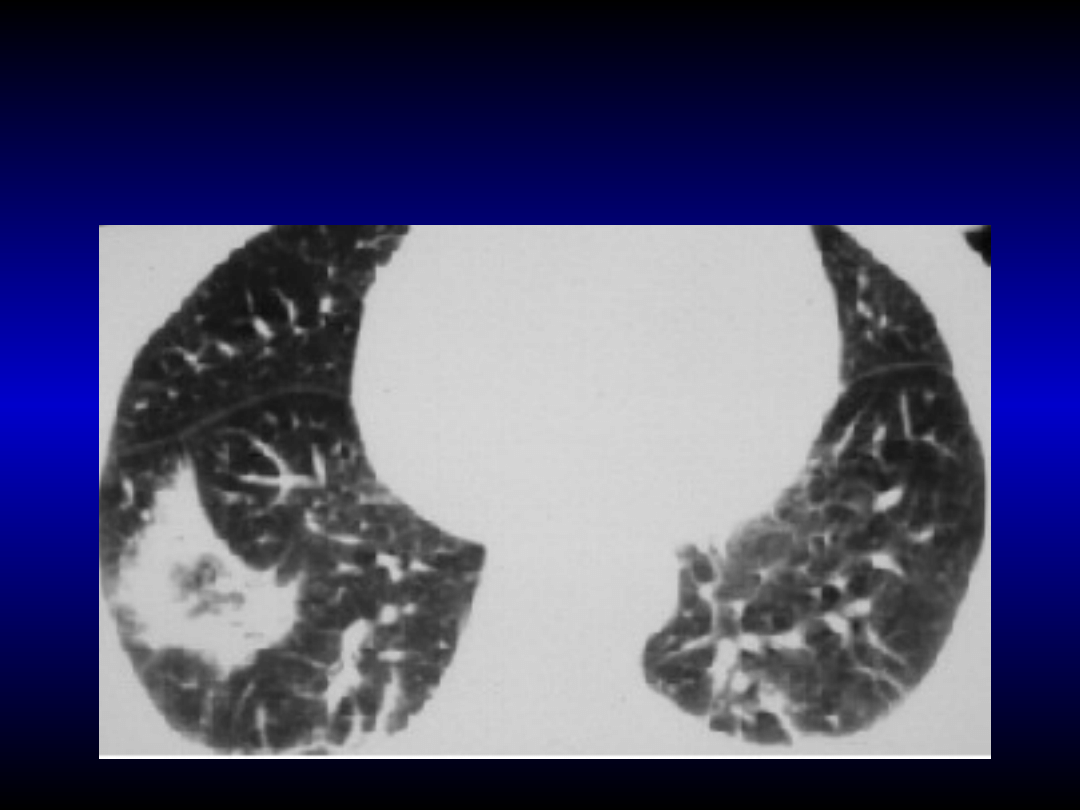
Pathologic mass with central necrosis in the
Pathologic mass with central necrosis in the
right lung. Enlargement of hilar and
right lung. Enlargement of hilar and
paratracheal lymph nodes
paratracheal lymph nodes
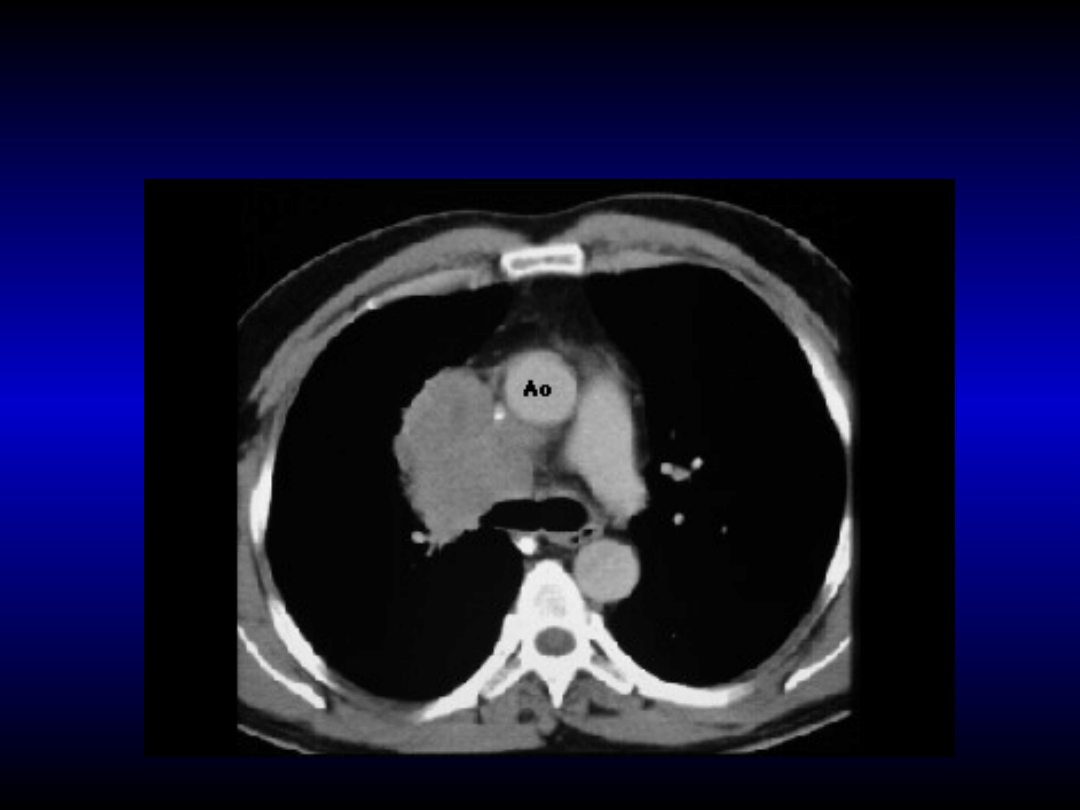
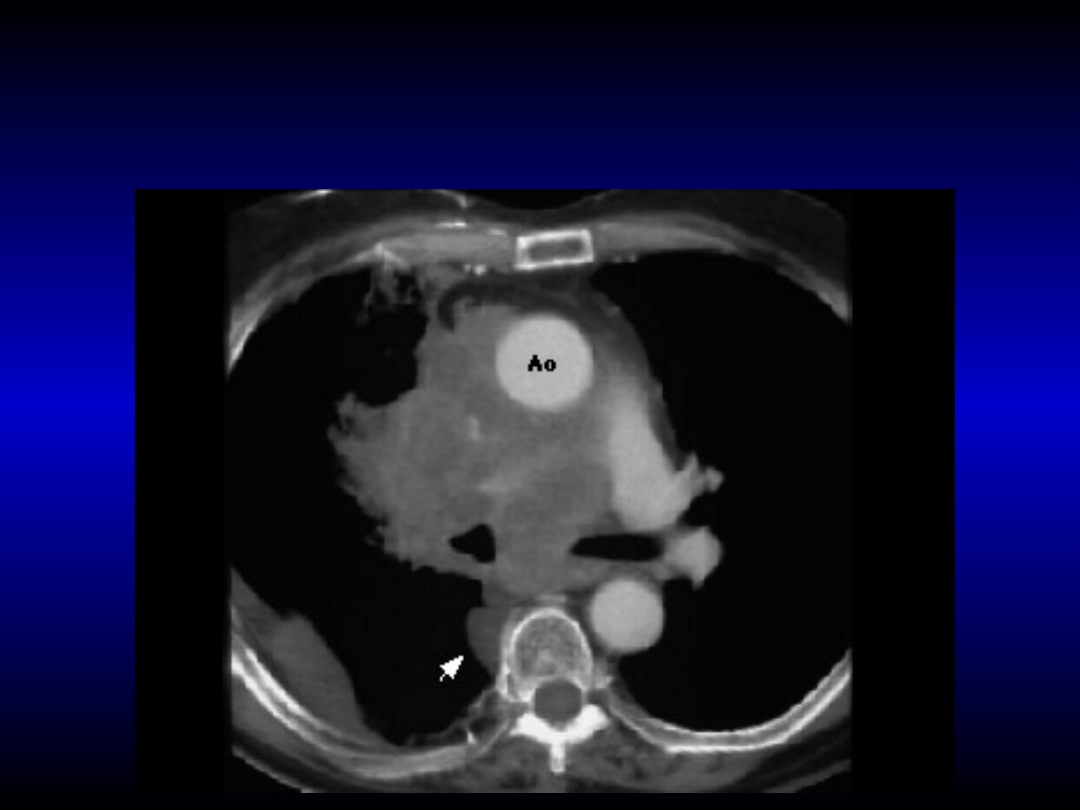
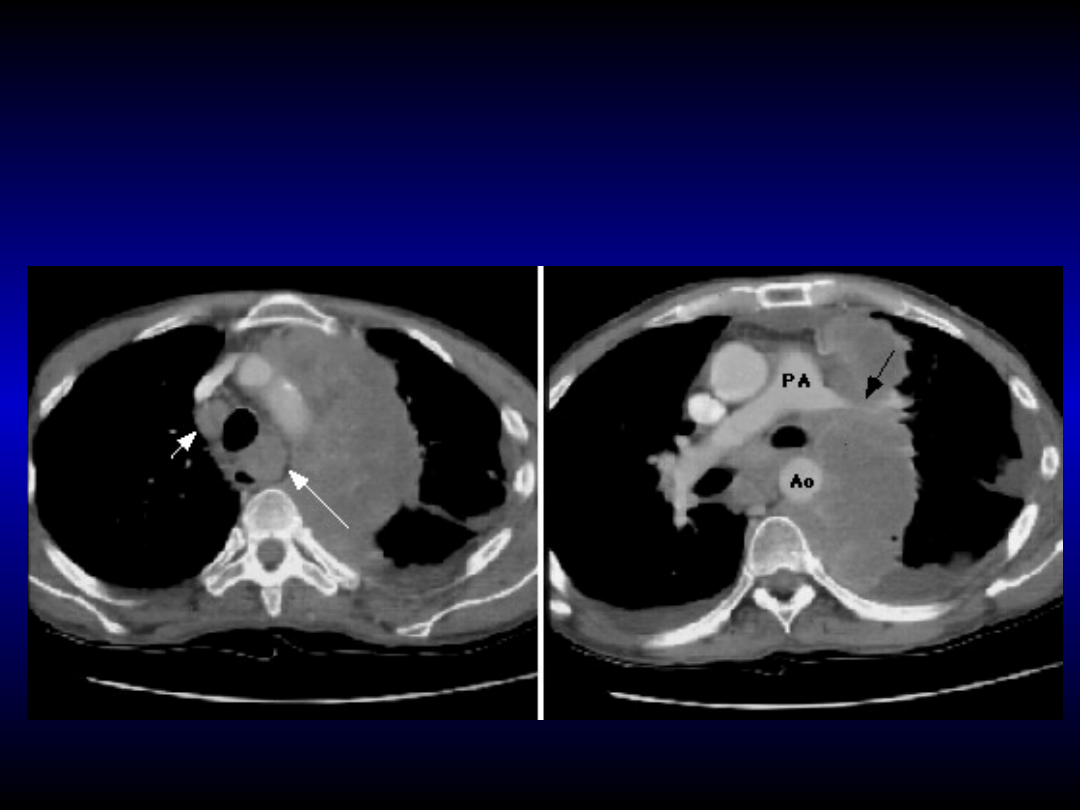
Small cell lung cancer with invasion to mediastinum.
Small cell lung cancer with invasion to mediastinum.
Infiltration of retroaortal space with superior caval
Infiltration of retroaortal space with superior caval
vein syndrome
vein syndrome
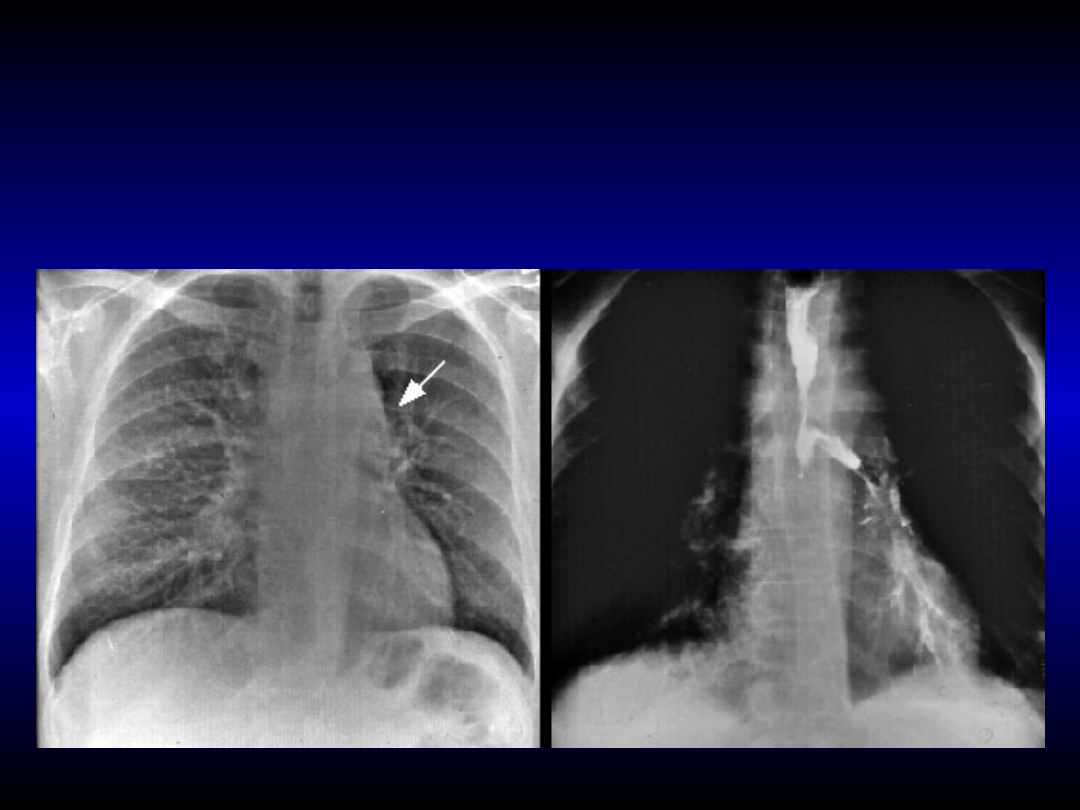
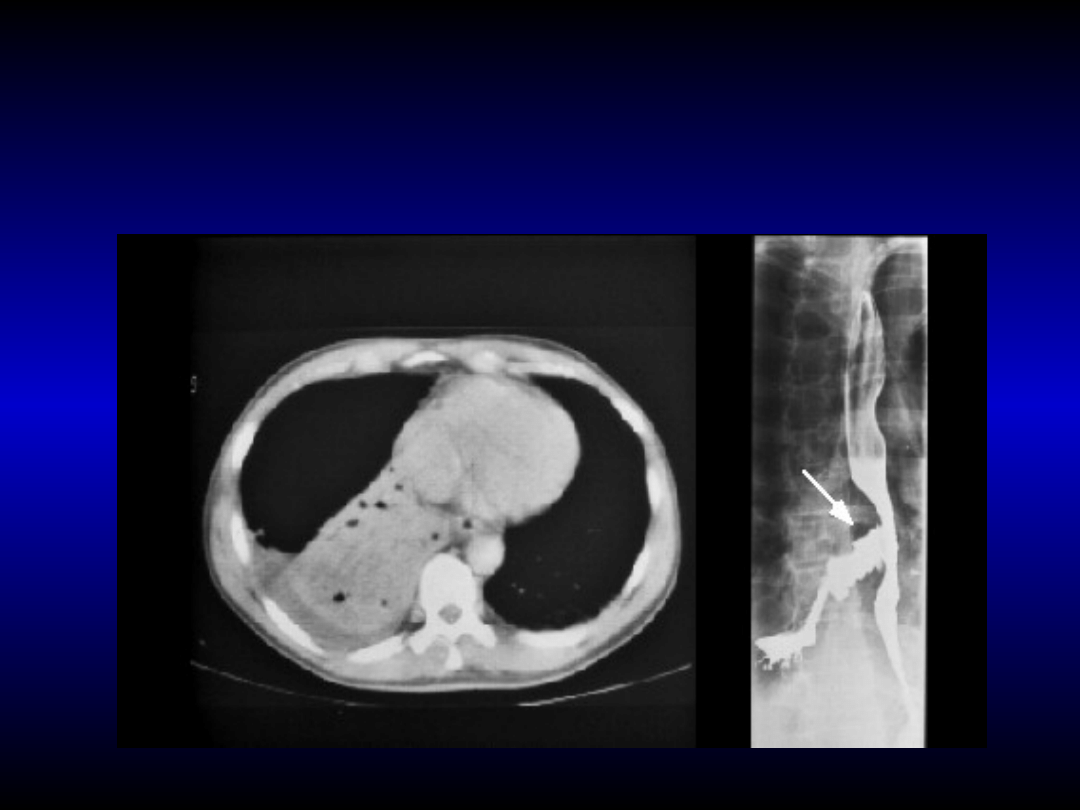
Lung cancer with infiltration of
Lung cancer with infiltration of
mediastinum and destruction of
mediastinum and destruction of
oesophagus wall (broncho-
oesophagus wall (broncho-
oesophageal fistula)
oesophageal fistula)
Lung cancer in the right main bronchus
Lung cancer in the right main bronchus
near tracheal bifurcation. Calcification in
near tracheal bifurcation. Calcification in
lymph nodes is characterised for earlier
lymph nodes is characterised for earlier
tuberculosis
tuberculosis
Adenocarcinoma of
Adenocarcinoma of
the
the
left
left
lung
lung
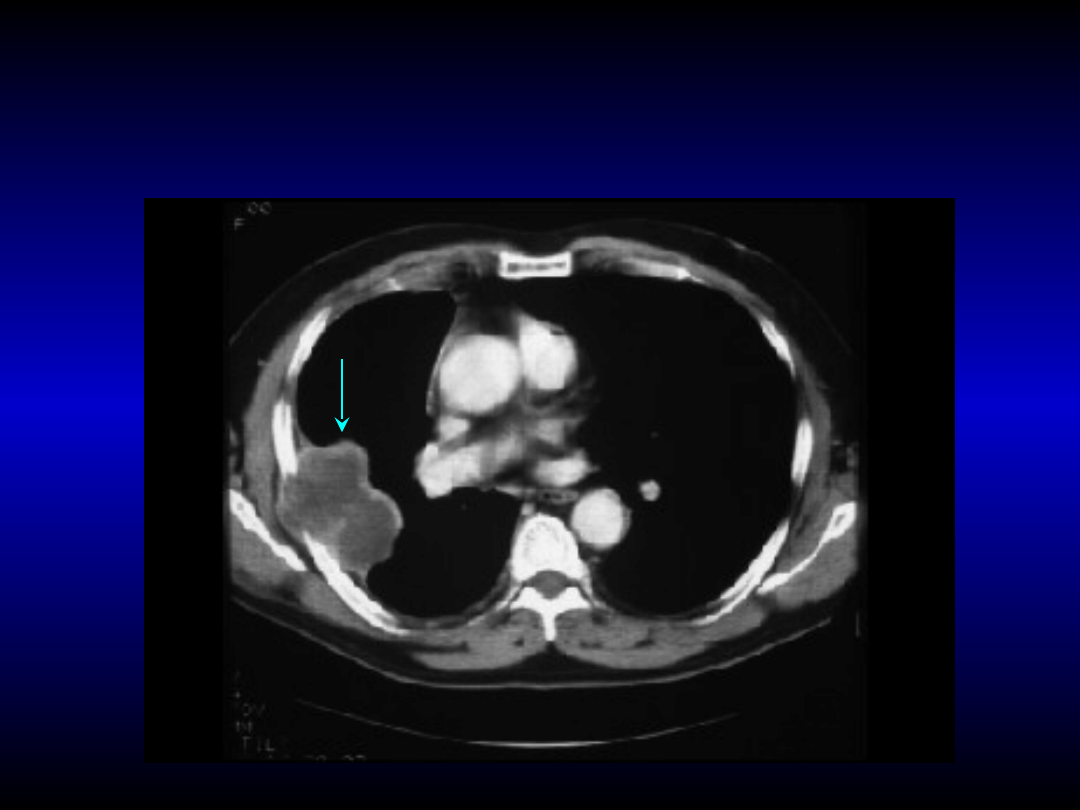
Adenocarcinoma
Adenocarcinoma
of peripheral part of
of peripheral part of
right lung with infiltration of thorax
right lung with infiltration of thorax
wall and ribs
wall and ribs
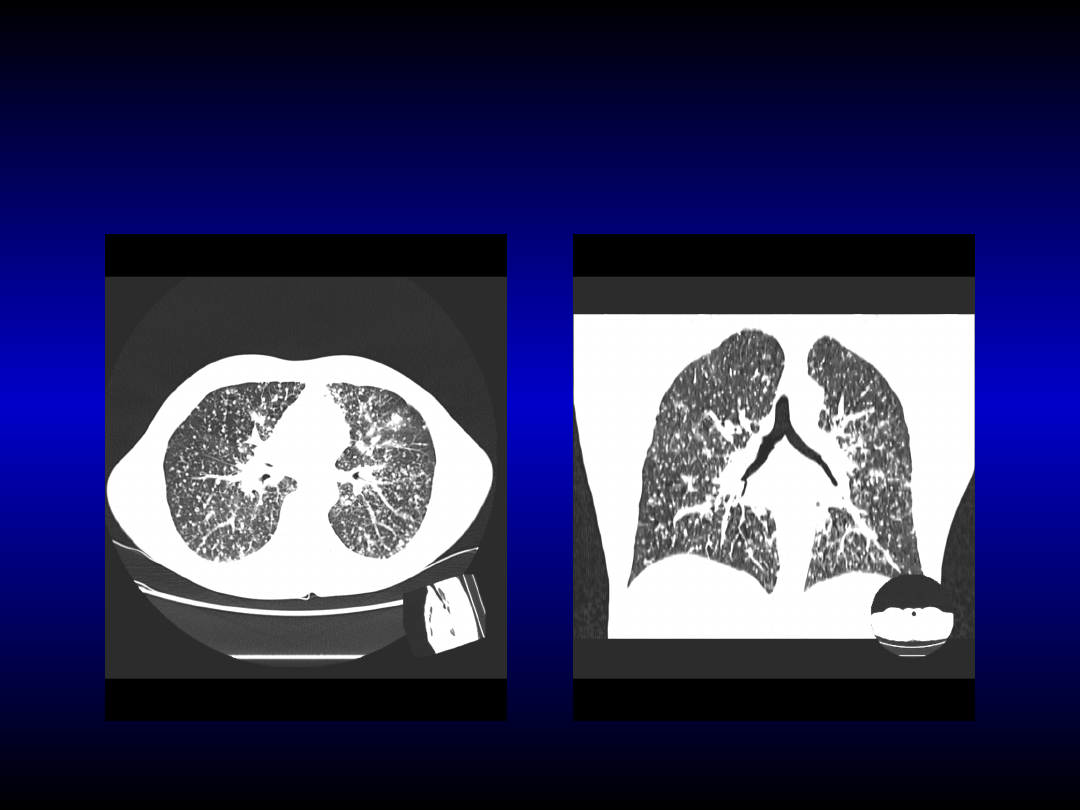
Multifocal infiltration
Multifocal infiltration
is
is
characterised for
characterised for
b
b
rochioloalveolar
rochioloalveolar
adenocarcinoma
adenocarcinoma

Pancoast’s tumor in apex
Pancoast’s tumor in apex
of right lung
of right lung

Pancoast’s tumor in MRI (infiltration
Pancoast’s tumor in MRI (infiltration
of thoracic vertebrae)
of thoracic vertebrae)

The clinical symptoms and
The clinical symptoms and
results of additional
results of additional
examinations, which may
examinations, which may
suggest diagnosis of lung
suggest diagnosis of lung
cancer, must be confirmed by
cancer, must be confirmed by
histopathology analysis of
histopathology analysis of
tissues specimens.
tissues specimens.

Diagnosis of lung cancer
Diagnosis of lung cancer
How to obtain pathological tissues?
How to obtain pathological tissues?
cytology of sputum;
bronchofiberoscopy:
• intrabronchial biopsy and exfoliative biopsy (sensitivity 55-85%);
• transbronchial biopsy (forceps biopsy, sensitivity 55-85%);
• transbronchial fin-needle biopsy with EBUS-FNA (sensitivity 90-100%);
• bronchoaspirate or bronchoalveolar lavage (BAL);
fin-needle aspiration biopsy by thorax wall (complication is pneumothorax,
which occurs in 7% of patients and in 46% patients with COPD;
biopsy of pleura, examination of pleural effusion (paracenthesis);
transcutaneous biopsy of lymph nodes, infiltrations of softy tissues,
metastases in liver, bones, bone marrow;
mediastinoscopy;
videothoracoscopy;
exploratory thoracotomy.

Sputum cytology
Sputum cytology
Sputum cytology have to be performed
Sputum cytology have to be performed
minimum 3 times
minimum 3 times
Sensitivity: 80% for central tumors
50% for peripheral tumors
Highest sensitivity for squamous cell carcinoma
Lowest sensitivity for adenocarcinoma

Imaging in lung cancer
Imaging in lung cancer
chest computed tomography;
abdominal ultrasonography and ultrasonography of pleural cavity;
abdominal computed tomography;
computed tomography of central nervous system;
magnetic resonance imaging of central nervous system and in the
tumor of chest wall as well as in the tumors with obturative
atelecatsis;
scintigraphy of sceleton;
contrast X-ray examination of oesophagus. Badania kontrastowe
przełyku jeżeli występują objawy ucisku.
PET scan (positron emission tomography scan): A fluorodoexyglucose
is injected intra venous. The PET scanner rotates around the body
and makes a picture of where glucose is being used in the body.
Malignant tumor cells show up brighter in the picture because they
are more active and take up more glucose than normal cells do.

The role of computed
The role of computed
tomography in lung cancer
tomography in lung cancer
diagnosis
diagnosis
staging in lung cancer: localisation and estimation of tumor
size, appearance of infiltration of pleura or mediastnal
organs, visualisation of enlargement lymph nodes in
mediastinum:
• qualification to surgical resection;
• planning of chemotherapy and radiotherapy (neoadivant, adiuvant
chemotherapy and chemotherapy and radiotherapy in locally advanced or
advanced non-small cell lung cancer.
planning of chemotherapy and radiotherapy in small cell lung
cancer;
estimation of responce on chemotherapy and radiotherapy;
information of reccurence or progression of disease.
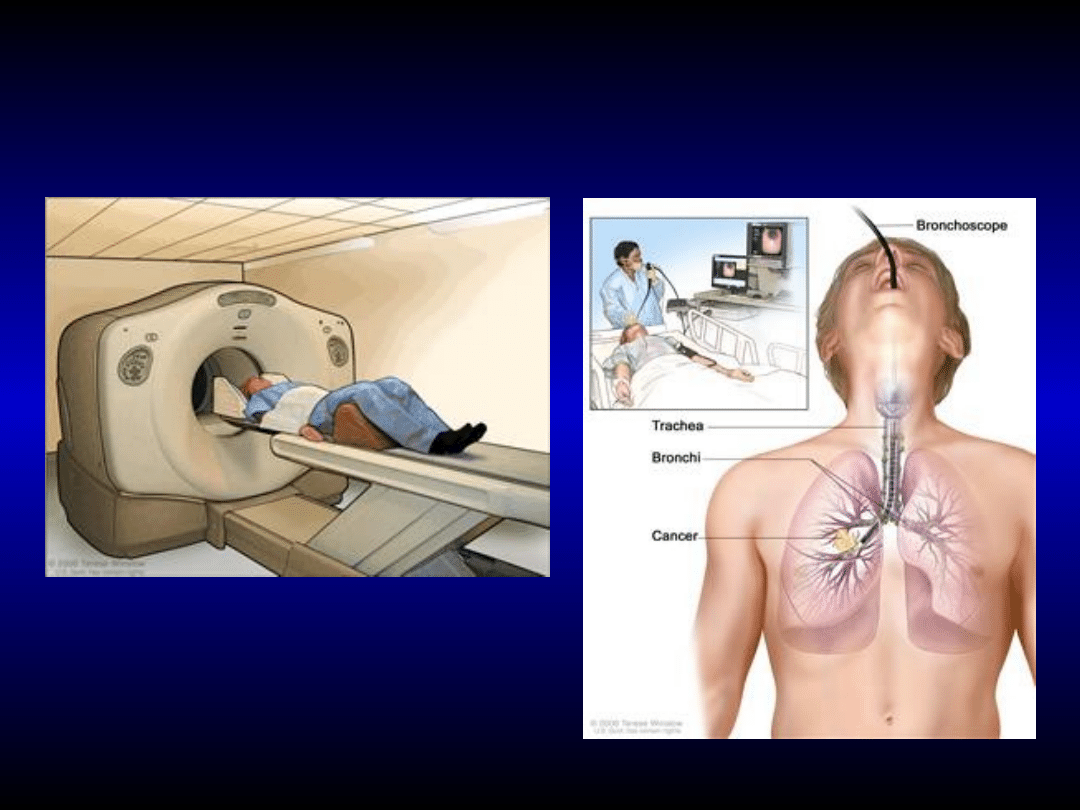
The main methods in lung
The main methods in lung
cancer diagnosis are:
cancer diagnosis are:
CT and PET
bronchoscopy

Staging in lung cancer
Staging in lung cancer
range of lung cancer (anatomical
staging)
• estimation of resection possibility
(computed tomography and MRI);
estimation of general condition -
possibility of surgical treatment
• estimation of operation possibility
(performance status, pulmonary
function tests, gasometry,
electrocardiography).
International TNM
International TNM
classification of lung
classification of lung
cancer
cancer
Stage
TNM
% of 5-years survival
I T1-T2 N0 M0
60-80
IIT1-T2 N1 M0
25-50
IIIA T3 N0-N1 M0 25-40
T1-T3 N2 M0
10-30
IIIB each T4 or
< 5
each N3 M0
IV
each M1 < 5

Gradation in small cell
Gradation in small cell
lung cancer
lung cancer
Localized disease (30%) -
unilateral process, which
occupied only regional lymph
nodes, eventually with metastases
to supraclavicular lymph nodes
and pleura. There is possibility of
application of high-voltage
radiotherapy.
Extensive disease (70%).
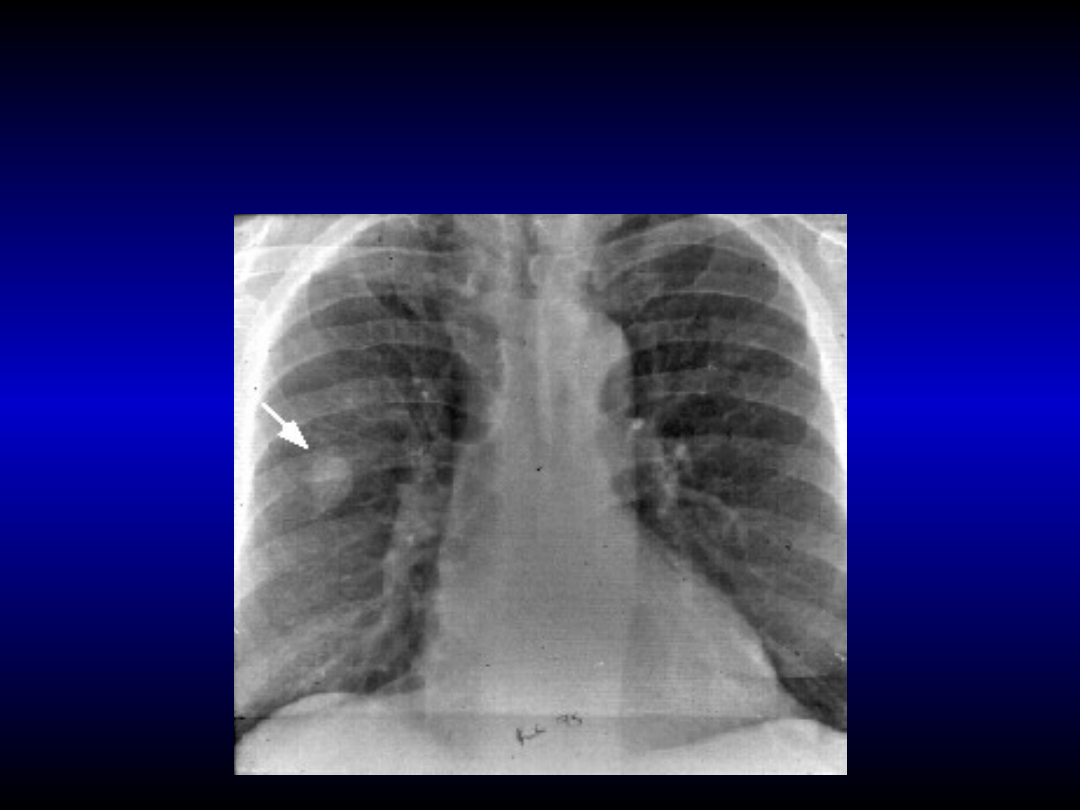
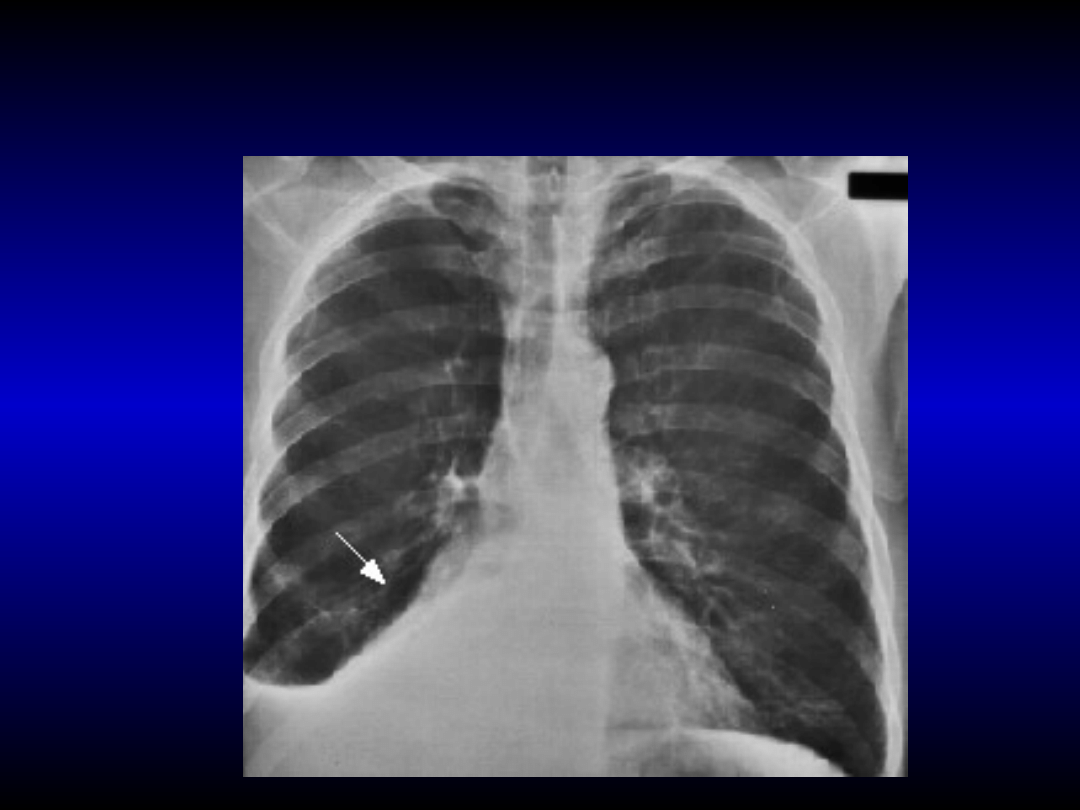
Solid infiltration (smaller than 3 cm) in inferior
Solid infiltration (smaller than 3 cm) in inferior
lobe
lobe
of right lung. Probable stage I of lung cancer
of right lung. Probable stage I of lung cancer
(T1 N0 M0)
(T1 N0 M0)
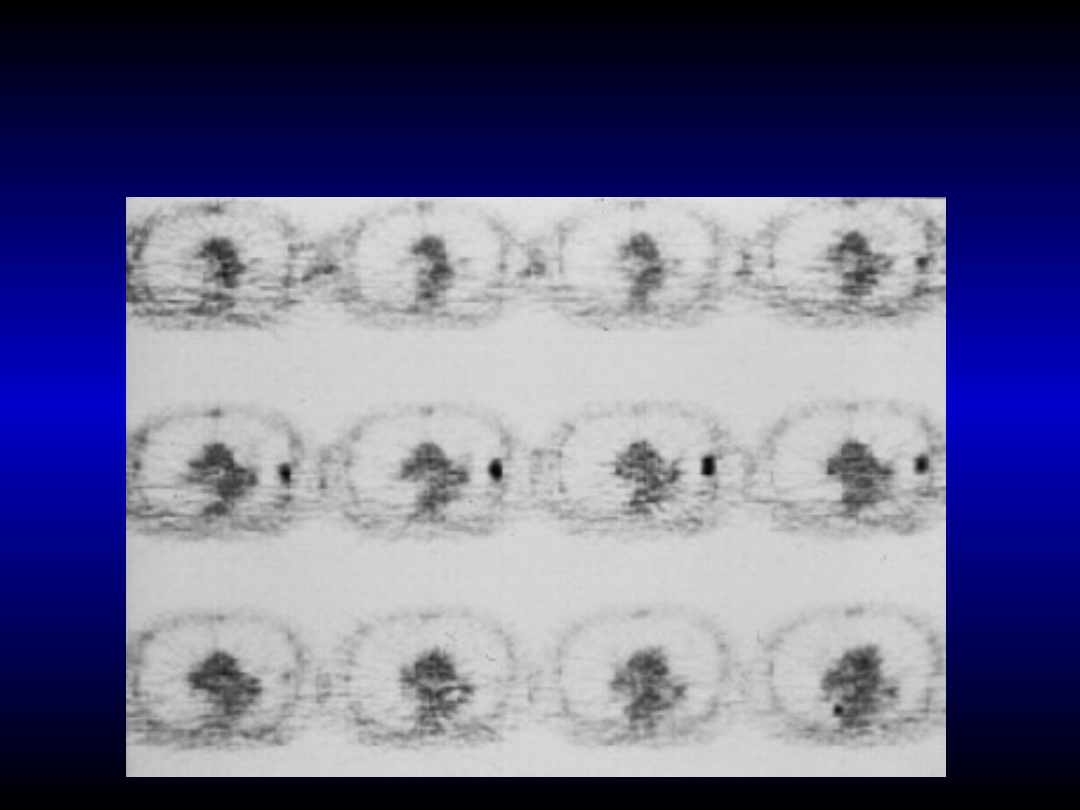
PET with fluorodeoxyglucose. Stage I (T1 N0
PET with fluorodeoxyglucose. Stage I (T1 N0
M0) of peripheral lung cancer in superior
M0) of peripheral lung cancer in superior
lobe of left lung
lobe of left lung
Brochioloalveolar adenocarcinoma
Brochioloalveolar adenocarcinoma
in stage
in stage
I (T2 N0 M0). Tumor of 3,5 cm size
I (T2 N0 M0). Tumor of 3,5 cm size
with central area of increased
with central area of increased
translucence
translucence
Lung cancer in stage II (T2 N1 M0) in
Lung cancer in stage II (T2 N1 M0) in
lingula of the left lung (size of 5 cm with
lingula of the left lung (size of 5 cm with
dystrophic calcification and
dystrophic calcification and
lymphadenopathy)
lymphadenopathy)
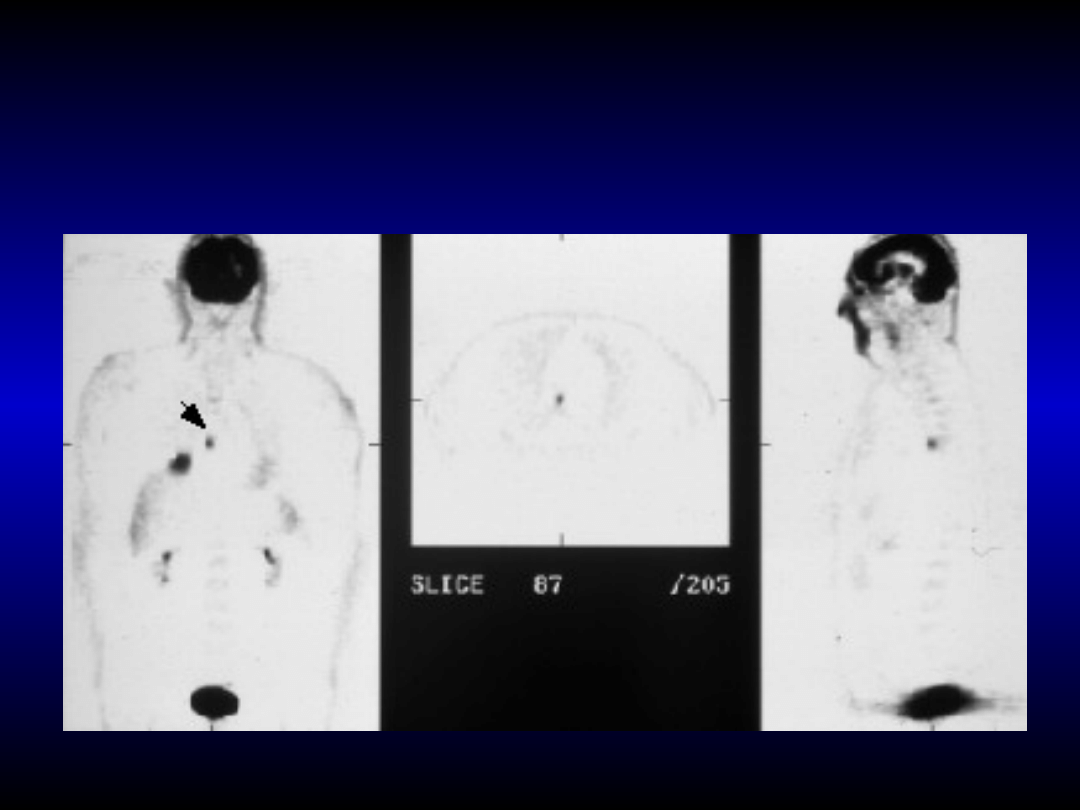
PET. Primary cancer
PET. Primary cancer
in
in
right lung and
right lung and
metastase in
metastase in
mediastinium lymph
mediastinium lymph
node
node
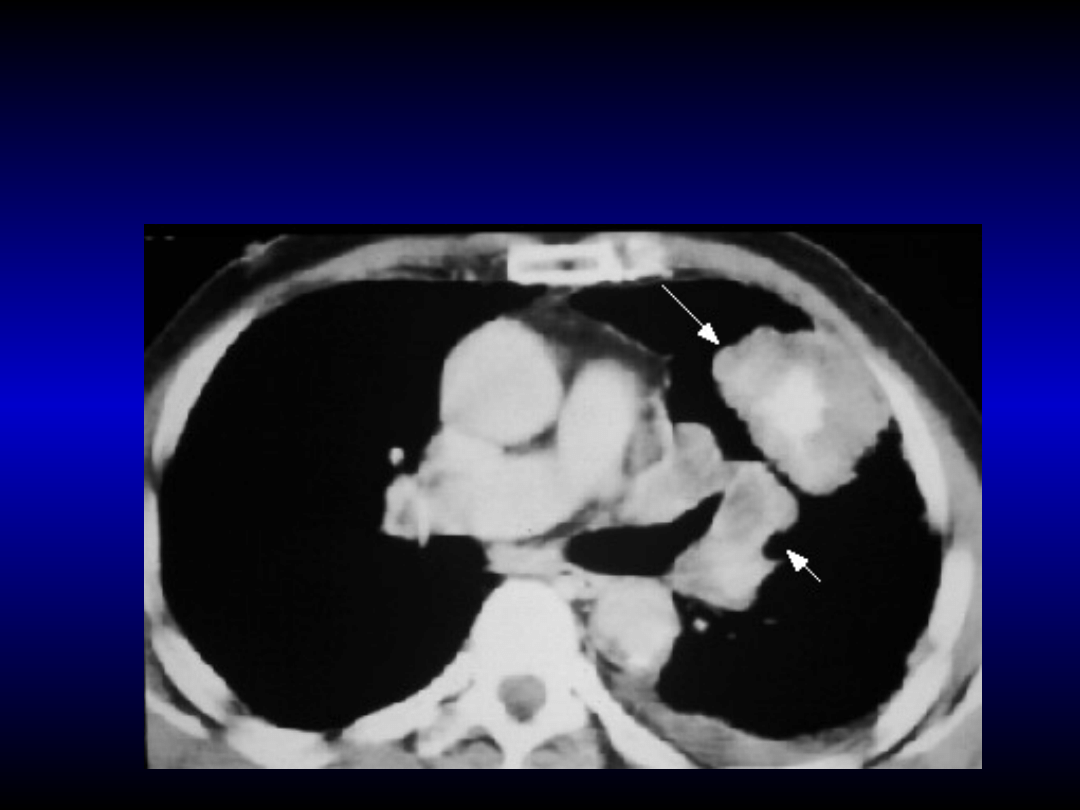
Small cell lung cancer infiltrating mediasti
Small cell lung cancer infiltrating mediasti
n
n
um.
um.
Enlargement of paravertebral lymph nodes.
Enlargement of paravertebral lymph nodes.
Stage IIIB (T4 N2 M0)
Stage IIIB (T4 N2 M0)
Lung cancer with infiltration of
Lung cancer with infiltration of
mediastinum and destruction of
mediastinum and destruction of
oesophagus wall (broncho-oesophageal
oesophagus wall (broncho-oesophageal
fistula). Stage IIIB (T4 N2 M0)
fistula). Stage IIIB (T4 N2 M0)
Adenocarcinoma of superior lobe of left lung.
Adenocarcinoma of superior lobe of left lung.
Infiltration of paratracheal lymph nodes, main
Infiltration of paratracheal lymph nodes, main
vessels and mediastinum lymph nodes on the
vessels and mediastinum lymph nodes on the
right side. Stage IIIB (T4 N3 M0)
right side. Stage IIIB (T4 N3 M0)

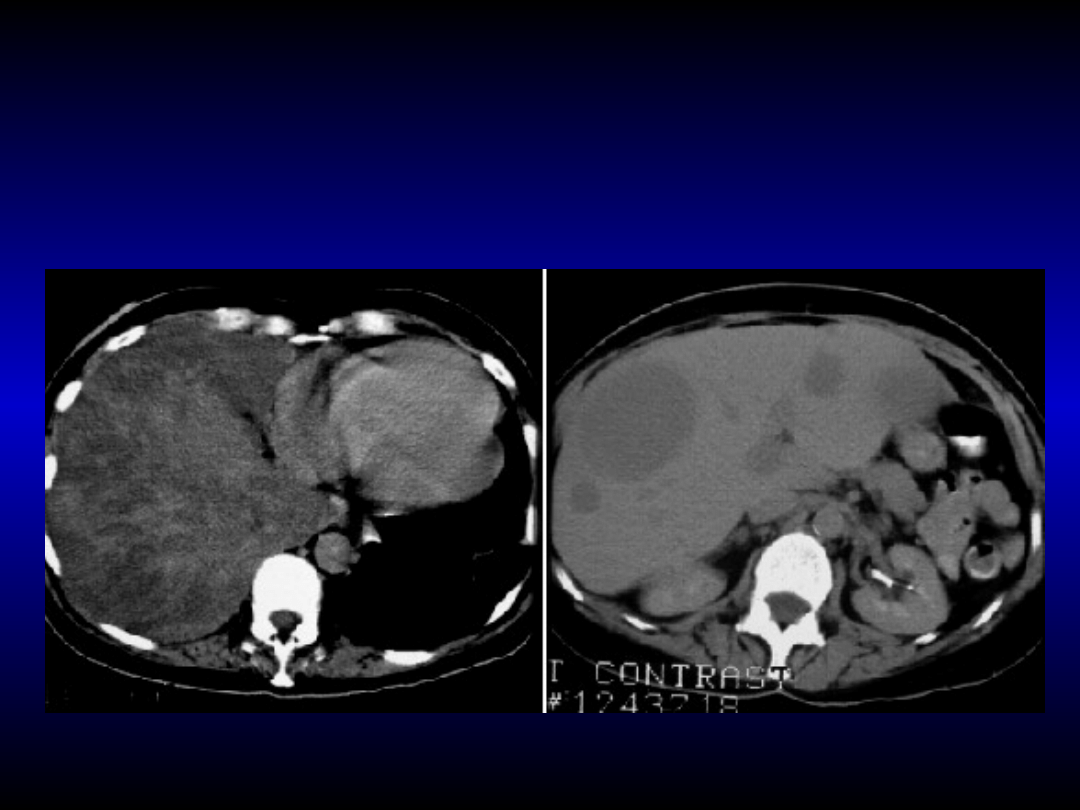
Lung cancer metastases –
Lung cancer metastases –
necrotic masses in left
necrotic masses in left
suprarenal gland and in
suprarenal gland and in
pancreas. Stage IV (M1)
pancreas. Stage IV (M1)
L
L
ung cancer
ung cancer
m
m
etastases
etastases
in
in
liver. Stage IV (T4 N3 M1)
liver. Stage IV (T4 N3 M1)
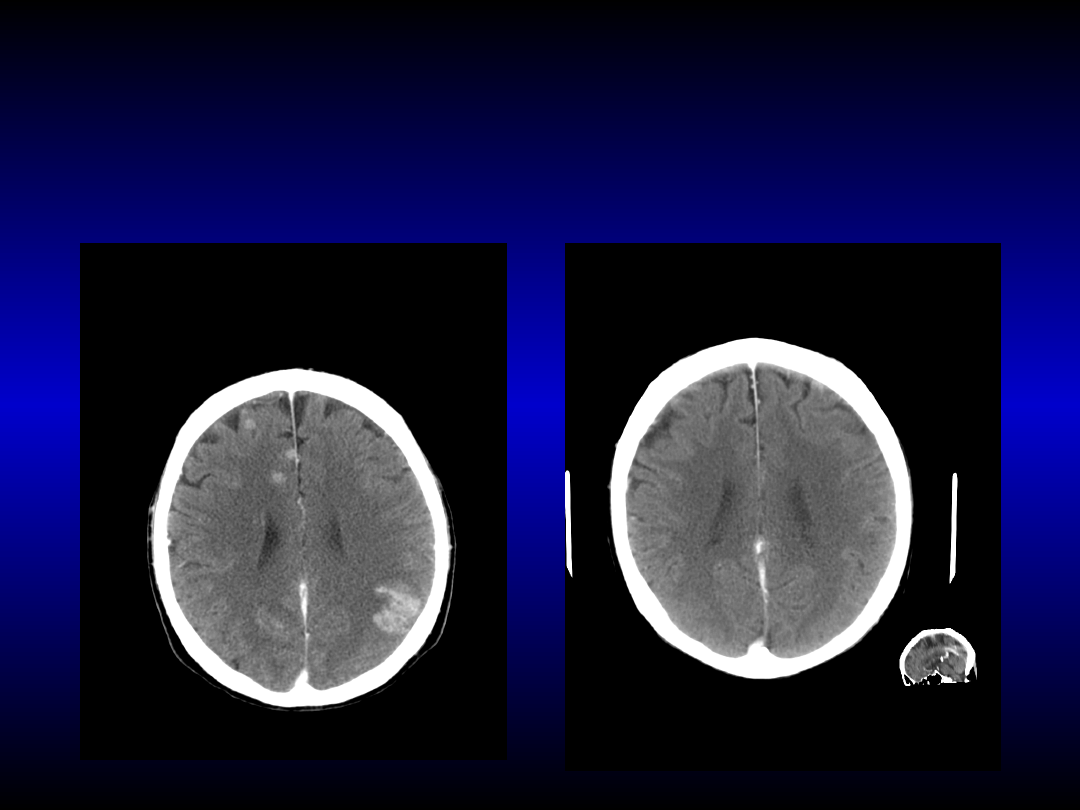
Adenocarcionoma metastases into brain
Adenocarcionoma metastases into brain
and their complete regression after
and their complete regression after
erlotinib treatment
erlotinib treatment

Mezothelioma
Mezothelioma
malignant neoplasm of pleura causing by exposition to
asbestos fibre (crocidolite) – occupational disease;
mezothelioma appears in two different forms: tumor
form or diffuse form;
rare metastases formation;
diagnosis:
• symptoms;
• chest X-ray and computed tomography;
• pleural biopsy and examination of pleural effusion;
treatment: surgical, radio- and brachytherapy,
chemotherapy (cisplatin + pemetrexed (Alimta
®
).
Mezothelioma
Mezothelioma

Pleural condensation and lack of
Pleural condensation and lack of
invasion in the chest wall typical for
invasion in the chest wall typical for
mezothelioma
mezothelioma

Benign noeplasms of
Benign noeplasms of
the lung
the lung
adenoma of bronchi:
• carcinoid from APUD cells and
carcinoid syndrome;
• cystadenoma;
• mucoepidermal tumor;
hammartoma, choristoma.
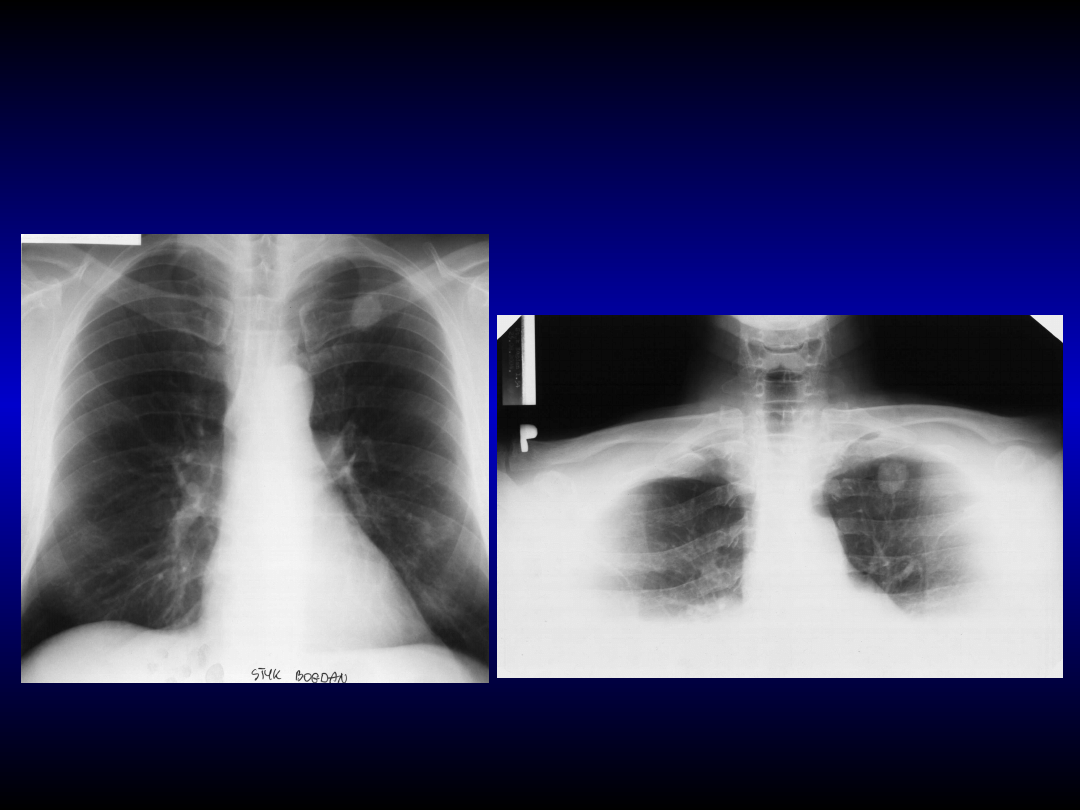
Hamartoma in „clavicular
Hamartoma in „clavicular
shadow”
shadow”
anteroposterior projection
oblique projection

Metastases to the lung
Metastases to the lung
in chest X-ray
in chest X-ray
examination:
examination:
breast round shadings
brain
reticulo-nodular shading
colon
nodular shading
with or
without disintegration
genitourinary system
adenopathy in
mediastinum and pleural effusion

Surgical treatment of non-small cell lung
Surgical treatment of non-small cell lung
cancer
cancer
I and II stages, and some IIIA stages:
surgical resection in stages I and II – lobectomy or pulmonectomy
(segmentectomy or wedge resection only in patients with bad condition);
survival time is more than 5 years for 50% of patients treated with radical
resection and more than 10 years for 15% of patients. Post-lobectomy mortality is
3%;
surgical resection with total removal of lymph nodes from mediastinum and
consideration for adjuvant chemotherapy in IIIA stage with N2 feature;
tumors with infiltration of chest wall (stage IIIB) - en block surgical
resection tumor and chest wall;
Pancoast’s tumor (T3 and stage IIIA) - en block resection of tumor
and chest wall, especially with intra-operation brachytherapy;
proximal infiltration of airway and N0 or N1 (stage IIIB) – cuff
resection or pulmonectomy with reanastomosis with opposite main
bronchus;
surgical resection of single metastases in central nervous system or
suprarenal glands and pulmonectomy of small primary tumors (stage
IV).
palliative surgical treatment (e.g. brain metastases).

respiratory and/or circulatory failure
connecting with COPD and other lung
diseases:
• total respiratory efficiency less than 40% of
normal value (FEV1 < 1 l);
• retention of carbon dioxide;
• pulmonary hypertension;
myocardial infarction in last 3 months;
arrhythmia;
poor performance status (PS = 3 or 4
points).
Contraindications to radical resection in lung
Contraindications to radical resection in lung
cancer - examination of patients’ general
cancer - examination of patients’ general
condition
condition

smoking;
patients older than 35 years;
tumor size larger than 6 cm;
lack of calcification;
symptoms suggested malignant neoplasm in chest;
attelectasis, pneumonia and/or hilar
lymphadenopathy in chest X-rays;
enlargement of tumor size in comparison with
previously chest X-rays.
The main risk factor supporting lung
The main risk factor supporting lung
resection in the suspicion of lung
resection in the suspicion of lung
cancer without confirmation in
cancer without confirmation in
histopathological diagnosis
histopathological diagnosis

Chemotherapy and radiotherapy
Chemotherapy and radiotherapy
in non-small cell lung cancer
in non-small cell lung cancer
neoadiuvant chemotherapy in patients with stage IIIA, if
surgical resection could be performed based on
mediastinoscopy results.
adjuvant chemotherapy in patients with stage IB, II and
IIIA after radical resection. Adjuvant radiotherapy may
be applied only in limited number of patients with stage
IIIA and N2 feature;
sequential or concurrent chemotherapy and radiotherapy
in patients with locally advanced NSCLC (stage IIIB);
first-line chemotherapy in patients with advanced NSCLC
(stage IIIB or IV);
second-line chemotherapy in patients with advanced
NSCLC and progression after first-line treatment;
third-line chemotherapy in patients with advanced
NSCLC and progression after first- and second-line
treatment;

Cytostatics and scheme of
Cytostatics and scheme of
treatment in non-small cell lung
treatment in non-small cell lung
cancer
cancer
First-line chemotherapy:
• Chemotherapeutic scheme involving two drugs based on
cisplatin or carboplatin and one of the following:
vinorelbine (Navelbine), gemcytabine (Gemzar), etoposid
(Vepesid), pemetrexed (Alimta) or docetaxel. These
scheme may be supplemented by bevacizumab (Avastin).
21-day cycles are used for various combination
chemotherapy regiments. The cycles are repeated twice
in neoadiuvant chemotherapy, 2-4 times in adiuvant
chemotherapy and up to 6 times in patients with
advanced NSCLC.
second-line chemotherapy:
• repeat of chemotherapy scheme if remission occured;
• monotherapy with pemetrexed, docetaxel or erlotinib.
third-line therapy with erlotinib.

Small cell lung cancer treatment
Small cell lung cancer treatment
sequential or concurrent multidrug chemotherapy and chest radiotherapy in patients with
localised disease and in good general condition;
multidrug chemotherapy in patients with extensive disease and in good general condition;
radiotherapy of central nervous system in the cases of metastases in brain or spinal cord in
limited or extensive disease;
palliative radiotherapy of distant metastases;
21-day cycles are used for various combination chemotherapy regiments. The cycles are repeated up to 6
times. Chemotherapeutic scheme involving following drugs
:
•
cisplatin or karboplatin with etoposide (Vepeside);
•
CAV scheme (endoxan, vinblastine, adriamycine);
in second-line chemotherapy, the scheme from first-line treatment should be used if remission
duration was more than 3 months. Topotecan (hycamtin) in monotherapy or another scheme
of chemotherapy should be used if early progression after first-line chemotherapy is noted
treatment effect:
•
clinical remission is noted in 30-50% of patients, disease progression in 10% of patients,
•
complete recovery is observed in 15-25% of patients with LD and in 1-5% of patients with ED;
•
survival time is 14-18 months for patients with limited disease and 10-12 for patients with extensive disease.
Survival time for untreated patients is 2-4 months.

relief of pain:
• nonsteroids anti-inflammatory drugs (NSAIDs);
• weak narcotic drugs with NSAIDs (codeine, tramal);
• narcotic drugs (Durogesic, morphine) with NSAIDs;
corticosteroids in limited number of patients;
counteraction of anorexia and effect of emaciation (Megace, hydration);
counteraction of infection due to granulocytopenic fever after
chemotherapy (rhG-CSF – Neupogen);
anemia controlling (erytropoietin – NeoRecormon, Darbopoietin);
vomiting controlling (Zofran, Atossa);
treatment of venous thromboembolic disease (low molecular weight
heparine - clexane);
treatment of bony pain and pathologic fracture (bisphosphonian - aredia);
antidepressive agents and psychotherapy;
brachytherapy;
palliative radiotherapy of metastases and infiltration of spine, bones,
central nervous system;
resection of life-threatening metastases (e.g. in central nervous system).
Symptomatic treatment in lung
Symptomatic treatment in lung
cancer
cancer
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
- Slide 26
- Slide 27
- Slide 28
- Slide 29
- Slide 30
- Slide 31
- Slide 32
- Slide 33
- Slide 34
- Slide 35
- Slide 36
- Slide 37
- Slide 38
- Slide 39
- Slide 40
- Slide 41
- Slide 42
- Slide 43
- Slide 44
- Slide 45
- Slide 46
- Slide 47
- Slide 48
- Slide 49
- Slide 50
- Slide 51
- Slide 52
- Slide 53
- Slide 54
- Slide 55
- Slide 56
- Slide 57
- Slide 58
- Slide 59
- Slide 60
- Slide 61
- Slide 62
- Slide 63
- Slide 64
- Slide 65
- Slide 66
- Slide 67
- Slide 68
- Slide 69
- Slide 70
- Slide 71
- Slide 72
- Slide 73
- Slide 74
Wyszukiwarka
Podobne podstrony:
ANGILESKI Lung Cancer
A review of the epidemiological evidence on tea, flavanoids, and lung cancer
socjalizacja uaktualniony materiał 19.05.2009, socjologia, soc małych gr i rodziny
Wykład 6 2009 Użytkowanie obiektu
Przygotowanie PRODUKCJI 2009 w1
Wielkanoc 2009
przepisy zeglarz 2009
Kształtowanie świadomości fonologicznej prezentacja 2009
zapotrzebowanie ustroju na skladniki odzywcze 12 01 2009 kurs dla pielegniarek (2)
perswazja wykład11 2009 Propaganda
Wzorniki cz 3 typy serii 2008 2009
2009 2010 Autorytet
Cw 1 Zdrowie i choroba 2009
download Prawo PrawoAW Prawo A W sem I rok akadem 2008 2009 Prezentacja prawo europejskie, A W ppt
Patologia przewodu pokarmowego CM UMK 2009
Wykład VIp OS 2009
2009 04 08 POZ 06id 26791 ppt
perswazja wykład1 2009 Wpływy w sferze społeczno politycznej
więcej podobnych podstron