
Rodzina
Enterobacteriaceae
Rodzaj: Salmonella,
Shigella, Proteus
General
characteristics
of Salmonella
spp.
Gram negative rod
Motile
Non - sporeforming
Do not ferment lactose
on MacConkey agar
Produce gas when
fermenting glucose
Produce H2S from
thiosulfate
Possess O, H, and Vi
(capsular) antigens
All bacteria from the genera
Salmonella belong to two main
species
1.
S. bongori (10 serotypes) – rare
2.
S. choleraesuis – it is divided into 6
subspecies:
S. choleraesuis subsp. arizonae
S. choleraesuis subsp. choleraesuis
S. choleraesuis subsp. diarizonae
S. choleraesuis subsp. houtenae
S. choleraesuis subsp. indica
S. choleraesuis subsp. salamae
Within those subspecies there are known
over 2500 serotypes that are named!

To S. choleraesuis subsp.
choleraesuis belong the most
common serotypes
S. enteritidis
S. typhi
S. paratyphi A, B or C
S. galinarum
In a special Kauffmann-White’s table
there are collected the schemes of
antigenic structure(depending on O and H
antigenes) for all bacteria from the genera
Salmonella

Determinants of Salmonella
pathogenicity
Endotoxin = LPS = lipopolysaccharide
(with an antigenic polysaccharide = antigen
O): fever, hypoglycemia,leucopenia,
hypotension,perfussion disturbances,
activation of C3 and complement,
disseminated intravascular clotting,shock
Invasins: proteins taking part in adherence to,
and penetration of, intestinal epithelial cells.
Factors involved in resistance to phagocytosis
Factors involved in resistance to acidic pH
Vi antigen (capsular polysaccharide with
antiphagocytic properties)

Epidemiology
Reservoir: animals
Invasion route: alimentary, fecal – oral
Portal of entry: epithelium of small intestine
Salmonellosis is usually caused by animal
pathogens that come to humans through
contaminated food ( poultry and eggs)
Typhoid fever and typhoid-like illness are
acquired via fecal-oral route, contaminated
water/food (asymptomatic chronic carriers –
they usually suffer from the disease of biliary
tract; bacteria live here and are excrete with
feces)

Pathogenesis of Salmonella
spp.
Mucosal penetration
Mucosal inflammation
(fluid and electrolyte loss)
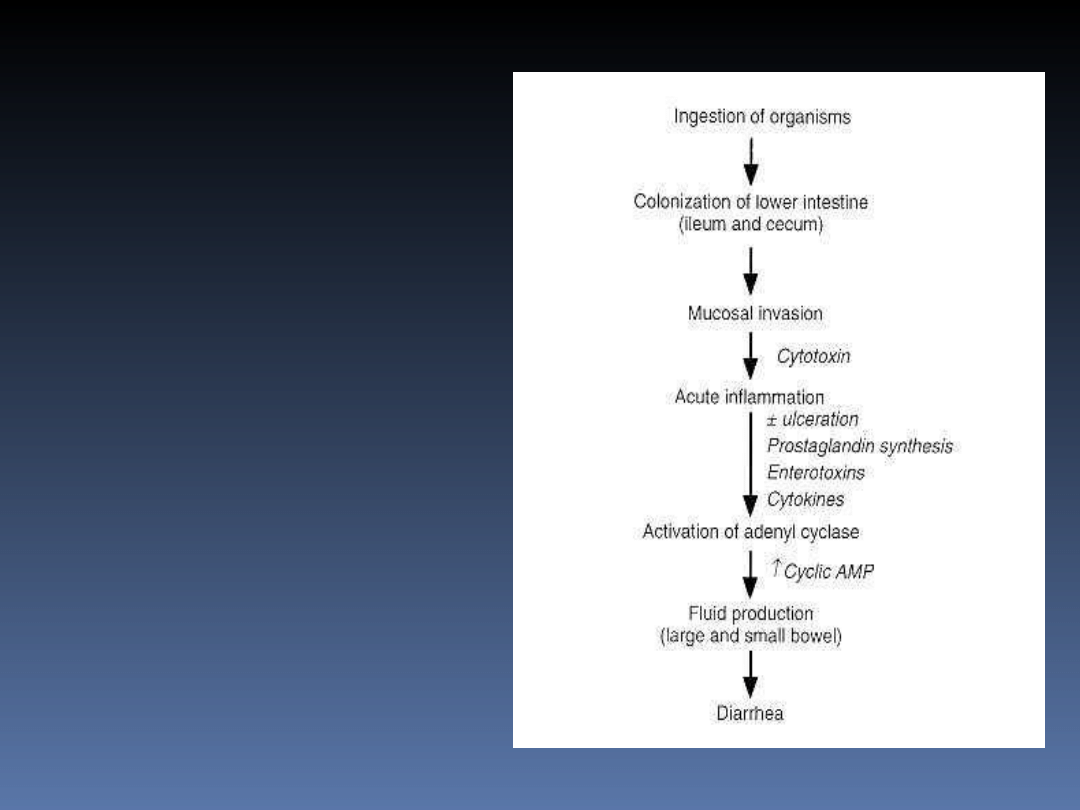
Pathogenesis
of Salmonella
enterocolitis
and diarrhea

Clinical diseases caused by
Salmonella spp.
Typhoid fever/typhus abdominalis (S. typhi)
I week: malaise, fever, aches, pains, constipation
II week: bacteremia (high fever), tender abdomen,
rose-colored spots on the skin, diarrhea;
severe complications are very possible!
Paratyphus/typhoid-like illn. (S.paratyphi ABC)
Gastroenteritis called salmonellosis
(other bacteria from the genera Salmonella, e. g.
S. enteritidis and S. typhimurium) – diarrhea, fever,
abdominal pain, self-limited, lasts 2-5 days;
dehydration and electrolyte imbalance!
Other (rarely): infections of urinary/respiratory
tracts, abscesses, bacteremia, sepsis

Materials for investigation
of Salmonella infections
In salmonellosis the best material for
investigation are feces; bacteria must
be isolated!
If typhoid fever or paratyphus are
suspected: blood culture, feces, urine;
in intestinal phase – a swab of the
ulcer;
bacteria must be isolated!
Culturing: McConkey, special media
(SS, SF)
After isolation of Salmonella
spp.
Biotyping (to assign isolated bacteria to
the genus/genera Salmonella) [API 20E]
Serotyping: confirmation, and assigning to
one of the serotypes by using commercially
prepared diagnostic serum with Salmonella
antisera (slide agglutination test) or on the
basis of the specific immune response of
the patient (the Widal test – 6th week of
infection:
Anti O >1:160 (1:200) or increaseing level-
active disease
Anti H > 1:50
Anti H > 1:200 and low level of anti O – after
vaccination or past disease)

Treatment of Salmonella
infection
Salmonellosis – supportive treatment
Typhoid fever:
I. Chloramphenicol(formerly)
II. Ampicillin and trimethoprim-
sulfamethoxasole (biliary circulation)
(this drugs are more safe so: as
alternative)
III. Quinolones (norfloxacin,
ciprofloxacin) [recent trials] (safe,
effective, biliary circ.)
Control and prevention
From SALMONELLOSIS
Sanitation, immunization of the
animals
that we eat, proper cooking of poultry
products and meat
From TYPHOID FEVER
Sanitation measures, personal hygiene
An effective vaccine is being sought
Characteristi
cs of
Shigella spp.
Gram negative rod
NONMOTILE
Do not ferment lactose
readily on MacConkey
agar
Do not produce gas
from fermentable
carbohydrates
Do not produce H
2
S
from thiosulfate

Classification of Shigella
species
S. dysenteriae (belongs to group A) (catalase-
negative, unlike other Enterobacteriaceae)
S. flexneri (belongs to group B)
S. boydii (belongs to group C)
S. sonnei (belongs to group D)
Because of the differences in somatic antigens
(antigens O) and in biochemical properties

Virulence factors of Shigella
spp.
LPS (irritable for intestines)
Invasion plasmid antigens (mediate
attachment to, and penetration of, mucosal
epithelial cells)
Intercellular spread proteins (they facilitate the
spread of bacteria from one cell to another)
SHIGA TOXIN (inhibition of protein synthesis
in humans – mucosal cells’ death); it is a
cytotoxic exotoxin produced only by S.
dysenteriae type 1 or 2 – it causes the most
severe infections

Epidemiology of Shigella
species
True human pathogen (no animal
reservoir)
Transmission: fecal-oral route (direct
contact with infected individual) or
contaminated food and water

Pathogenesis
Ingestion of
organism
Colonisation of large intestine
Micro- abscess
formation
Necrosis of mucosa and superficial
ulceration covered with
pseudomembrane
During recovery – granulation tissue
and scars appear

Clinical diseases caused
by Shigella spp.
Bacterial dysentery/dysenteria
bacilliaris/ shigellosis
(severe abdominal cramps and
frequent, painful passage of low-
volume stools with blood and mucus)
Watery diarrhea (relatively mild
infection)
Gastroenteritis

Shigella dysenteriae
type 1 or 2
Produces Shiga toxin
This toxin causes the hemolytic-uremic
syndrome (disseminated endothelial
damage, leading to intravascular
clotting, hemolysis, and renal failure)
Diagnostics of
shigellosis
Bacteria must be isolated from feces or
rectal swabs
Biotyping (to assign isolated bacteria to
the genus Shigella)
Serotyping: confirmation, and assigning to
one of the subgroups (A/B/C/D) = species
by using samples of serum with various
antibodies for subgroup antigens and
antibodies peculiar to serotypes
(commercially prepared) – latex tests or
slide agglutination tests (to show the
table)

Treatment of shigellosis
Supportive therapy
Antibiotics can be given
(ampicillin, amoxicillin, trimethoprim-
sulfamethoxasole, ciprofloxacin,
azithromycin)
(widespread antibiotic resistance)
Prevention: sanitation and personal
hygiene (because of the fecal-oral
chain of transmission – feces, flies,
fingers)
Proteus genus
Members: P. vulgaris, P.
mirabilis, P.
myxofaciens, P. penneri
Extremely motile
(swarming colonies)
Generally produce
urease (ammonia
creation)
Possess O, H, and K
antigens
Used in Weil-Felix test
(to recognize rickettsiae
infection)

Patogenicity
Virulent factor: endotoxin
Clinical diseases:
Urinary tract infections (kidney stones)
Wound infections,
Septicemia
Food poisoning and diarhhea in neonates
Meningitis
Otitis media

Bacteriological
diagnosis
Speciment: urine, stools, pus, csfluid
Slide (Gram staining)
Culture on McConkey agar, blood agar,
agar (on agar growth H)
Identification :API, ATB
Document Outline
- Slide 1
- Slide 2
- Slide 3
- Slide 4
- Slide 5
- Slide 6
- Slide 7
- Slide 8
- Slide 9
- Slide 10
- Slide 11
- Slide 12
- Slide 13
- Slide 14
- Slide 15
- Slide 16
- Slide 17
- Slide 18
- Slide 19
- Slide 20
- Slide 21
- Slide 22
- Slide 23
- Slide 24
- Slide 25
Wyszukiwarka
Podobne podstrony:
Salmonella, Shigella, Yersinia A Deptuła 2007 CM UMK
Salmonella, Shigella, Yersinia A Deptuła 2007 CM UMK
SALMONELLA i SHIGELLA
Salmonella, Shigella, Yersinia
Salmonella arizonae
PROTEUS2008 09 11
Salmonella
SALMONELLOZY ZWIERZíT TOWARZYSZíCYCH
Salmonella 2
SALMONELLOZY I CZERWONKA
3 Shigella
Salmonelloza
salmonella i e coli
SALMONELLA (1)
Salmonelloza
bakterie wykłady, 1. E.coli, (salmonella), Mikrobiologia 3
Salmonella to pałeczki jelitowe Gram
więcej podobnych podstron